
Clinical Observation on Acupoint Sticking Therapy for Lumbar Intervertebral Disc Hernination
2013-07-18 11:57:23ZhengZhaojianLinLianbing
Zheng Zhao-jian, Lin Lian-bing
1 Wenling Municipal No.1 People’s Hospital, Zhejiang 317500, China
2 Wenling Municipal No.3 People’s Hospital, Zhejiang 317523, China
Clinical Observation on Acupoint Sticking Therapy for Lumbar Intervertebral Disc Hernination
Zheng Zhao-jian1, Lin Lian-bing2
1 Wenling Municipal No.1 People’s Hospital, Zhejiang 317500, China
2 Wenling Municipal No.3 People’s Hospital, Zhejiang 317523, China
Objective: To observe the clinical effects of acupoint sticking therapy for lumbar intervertebral disc herniation.
Methods: Seventy patients with lumbar intervertebral disc herniation were randomly divided into two groups by the visit order, 35 cases in each group. The treatment group was treated with acupoint sticking therapy and the control group was treated with tuina. After treatment, the clinical effects, pain integral and Japanese Orthopedic Association (JOA) scores were compared between the two groups.
Results: The total effective rate, pain integral and improvement of JOA scores were better in the treatment group than in the control group (P<0.05).
Conclusion: Acupoint sticking therapy is affirmative in the therapeutic effects and better than tuina treatment for lumbar intervertebral disc herniation.
Acupoint Sticking Therapy; Intervertebral Disc Displacement; Massage; Tuina; Low Back Pain
Lumbar intervertebral disc herniation (LIDH) is a common and intractable disease. There are numerous conservative methods for LIDH. Many methods were reported ‘magic’ in the therapeutic effects, but have not been confirmed by scientific study. In various non-surgical therapies, as one of the effective conservative methods for LIDH, Chinese medical therapy has been extensively applied in the clinical treatment. But its concrete application is still quite blind and random. This influenced the improvement of clinical effects and development of this subject. Due to improper selection of the therapeutic methods, some patients develop chronic LIDH, leading to inconvenience to their life and work. From July of 2010 to January of 2012, we treated 35 cases of LIDH patients with the acupoint sticking therapy, in comparison of the clinical effects with 35 cases treated by tuina.
1 Clinical Materials
1.1 Diagnostic criteria
In reference to the diagnostic criteria in theLumbar Intervertebral Disc Herniation[1]and theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[2], there was a history of traumatic injury in the low back, chronic strain or cold and dampness exposure, and chronic history of low back pain before the onset in most patients. It often occurs in the young and middle-aged adults, with pain radiating from the low back to the hip and lower limb, and pain aggravated byincreasing abdominal pressure (cough, sneezing), accompanied by lateral bending of the spine, disappearance of the physiological curve of the low back, tenderness next to the involved spinous process, radiating to the lower limb and leading to the motor limitation in the low back. Insensitivity may exist in the involved innervations of the lower limb, and the muscular atrophy may occur in the patients with long duration. Straight leg-raising test or intensified test is positive, and the knee and Achilles reflex decreases or disappears, and the extending power of the big toe declines. The anterior-posterior and lateral X-ray films in the imaging examination showed the changes of the physiological curve and intervertebral space in the varying degrees, and hyperosteogeny on the border of the adjacent vertebrae. CT examination may show the location and extent of disc herniation.
1.2 Inclusion criteria
Those who were in conformity with the diagnostic criteria of disc herniation; with the age ranging from 15-75 years old; male or female; stopped other therapies during the treatment of this method; willing to attend this trial and signed informed consent.
1.3 Exclusion criteria
Those who were not in conformity with the abovementioned diagnostic criteria; those complicated with primary diseases seriously endangering the life in the cardiocerebrovascular, hepatic, renal and hematopoietic system, and sick with mental disorders; woman in pregnancy; patients were sick with spinal inflammatory lesions, such as tuberculosis, rheumatoid and proliferative lesions, and sick with spinal fracture in various parts; hypertrophy of yellow ligament, truck sciatica, piriformis syndrome, injury of superior clunial nerves; congenital or secondary spinal stenosis; tumor of cauda equina, congestion of the intervertebral venous plexus, radiculitis, thromboangiitis obliterans, spondyloschisis, spondylolisthesis; and those who accepted other treatments.
1.4 General data
Totally 70 cases were enrolled, after LIDH was diagnosed by CT or MRI. They were randomly divided into a treatment group and a control group by the visit orders, 35 cases in each group. There were 16 males and 19 females in the treatment group, with the age ranging from 18 to 65 years old, at the average age of 46.2, and duration ranging from 2 h to 6.2 years, at the average of 135 d. There were 15 males and 20 females in the control group, with the age ranging from 20 to 62 years old, at the average age of 46.4, and duration ranging from 10 h to 7.5 years, at the average of 139 d. The gender, age and duration in the patients of the two groups were not statistically significant (P>0.05), indicating that the two groups were comparable.
The clinical managements of the two groups are shown in Fig.1.
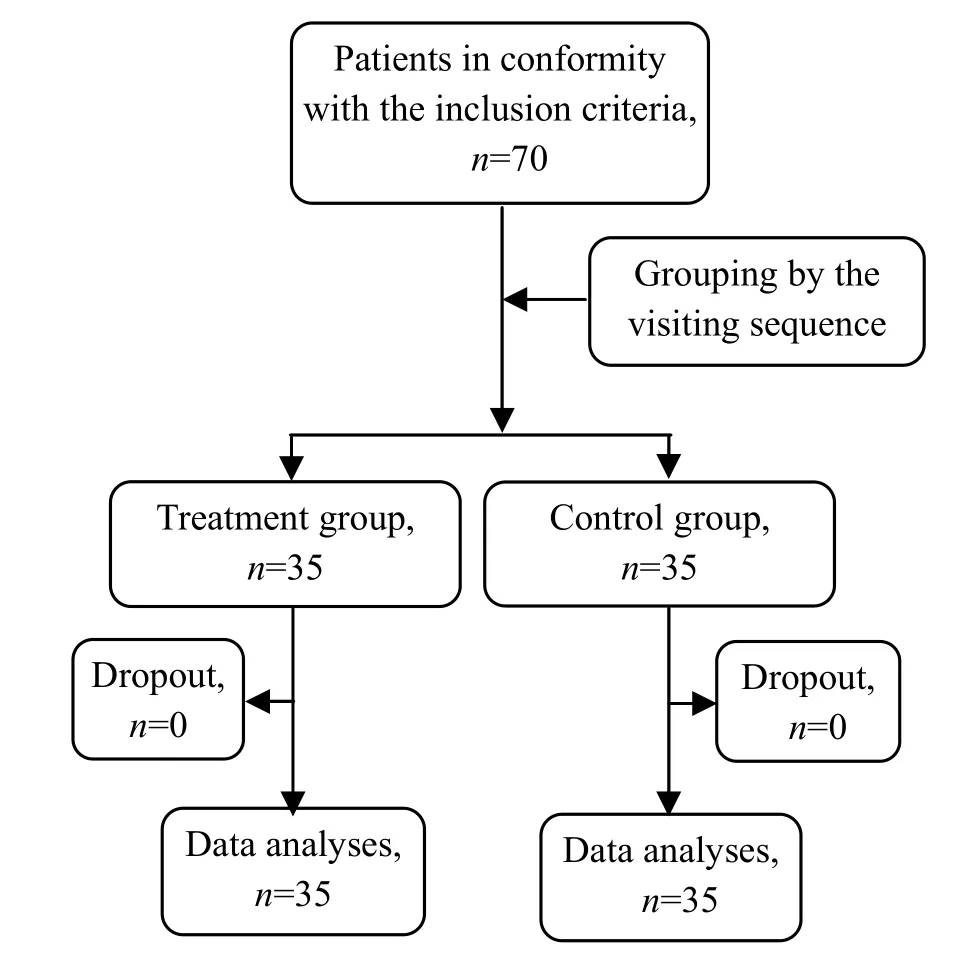
Fig.1 Procedure of clinical management
2 Therapeutic Methods
2.1 Treatment group
The patients in the treatment group were treated by external application of herbal drugs on the acupoints.
2.1.1 Herbal composition and manufacturing method
Herbal composition:Tian Nan Xing(Rhizoma Arisaematis) 30 g,Cao Wu(Radix Aconiti Kusenzoffii) 30 g,Xi Xin(Herba Asari) 10 g,Chuan Xiong (Rhizoma Chuanxiong) 10 g,Tao Ren(Semen Persicae) 12 g,Hong Hua(Flos Carthami) 12 g,Wu Ling Zhi(Faeces Trogopterorum) 10 g,Mo Yao(Myrrha) 12 g,Dan Shen(Radix Salviae Miltiorrhizae) 10 g,Qin Jiao(Radix Gentianae Macrophyllae) 15 g,Xiang Fu(Rhizoma Cyperi) 10 g,Di Long(Lumbricus) 10 g,Chuan Niu Xi(Radix Cyathulae) 10 g,Huang Qi(Radix Astragali) 50 g,Chuan Wu(Radix Aconiti) 30 g,Chi Shao(Radix Paeoniae Rubra) 10 g,Du Huo(Radix Angelicae Pubescentis) 10 g,Fang Feng(Radix Ledebouriellae) 10 g,Sang Ji Sheng(Ramulus Loranthi) 15 g,Du Zhong(Cortex Eucommiae) 12 g,Yan Hu Suo(Rhizoma Corydalis) 15 g,Tou Gu Cao(Herba Speranskia Tuberculata) 10 g,Bing Pian(Borneolum Syntheticum) 3 g,Dang Gui(Radix Angelicae Sinensis) 10 g,Mu Gua(Fructus Chaenomelis) 10 g,Jiu Da Huang(Rhizoma Rhei) (processed with wine) 50 g,Bi Ma You(Oleum Ricinus communis) 15 mL,Feng La(Cera Flava) 20 g,Song Xiang(Colophonium) 200 g,Bo He Bing(Mentholum) 3 g, Polyisobutylene 100 g.
Manufacturing method: Cataplasmata is manufactured by pharmacist of the hospital strictly based upon the manufacturing method of traditional Chinese medicine cataplasmata. Namely, the herbal stuffs ofTian Nan Xing(Rhizoma Arisaematis),Cao Wu(Radix Aconiti Kusenzoffii),Xi Xin(Herba Asari), andChuang Xiong(Rhizoma Ligustici Chuanxiong) are ground into coarse powder and extracted with percolation and condensed into the extract. Then, the extract is mixed withBo He Bing(Mentholum), dimethyl sulfoxide, vinegar, evergreen oil,Bing Pian(Borneolum Syntheticum), andSong Xiang(Colophonium) into active ingredients, and prepared into the matrix with polyisobutylene, sodium carboxymethyl cellulose, gelatin, glycerol,Bi Ma You(Oleum Ricinus communis), sorbitol, and proper amount of purified water. The above active ingredients were added proportionally with the percutaneous and absorbing enhancers (Azone 3 mL), and then added with the matrix and evenly smeared on the non-woven base material in 10 cm × 10 cm, and covered with protective film. After it is manufactured, it is cut into the small pieces in 2 cm × 2 cm, i.e. cataplasmata.
2.1.2 Acupoint sticking method
Acupoints: Bilateral Shenshu (BL 23), Yaoyangguan (GV 3), Chengshan (BL 57), Yanglingquan (GB 34), and Ashi point.
Operation: After the patient lied on the bed, cataplasmata was adhered on the above acupoints. The treatment was given once every day, for 16 h each time, and five days made one course. There was a two-day interval between the two courses, and totally four courses were given.
2.2 Control group
Tuina treatment was given to the patients in the control group.
The treatment was given in accordance with the operative method described inScience of Tuina[3], with the therapeutic principle to relax the tendons and dredge the collaterals, dredge the meridians and stop pain, regulate the tendons for restoration, and warm the kidney and strengthen the low back.
The lumbar region, back, hip and posterior aspect of the sick limb were Gun-Rolled, An-Pressed and Rou-Kneaded for no less than 10 min. Shenshu (BL 23), Pangguangshu (BL 28), Guanyuanshu (BL 26), Yaoyan (EX-B 7), Huantiao (GB 30), Chengfu (BL 36), Weizhong (BL 40), and Chengshan (BL 57) were An-Pressed and Rou-Kneaded for one 1 min at each acupoint. The oblique Ban-Pulling method of the low back, the straight leg-raising and Ban-Pulling method for the sick lower limb and the backward-stretching method of the low back were also applied. Shenshu (BL 23) and lumbosacral region were Ca-Rubbed. The low back was Yao-Shaken and the back, low back, hip and posterior aspect of the lower limb were Pai-Patted and Ji-Hit. If numb sensation is strong in the posterior aspect of the leg, dorsum of the foot, heel or sole, the lateral aspect of the leg was Tui-Pushed with the elbow, and the straight leg was raised and the foot was straightened for 5 times.
The treatment was given every day, for 20 min each time, and five days made one course. There was a two-day interval between the two courses, and totally four courses were given.
3 Observation on Effects
3.1 Statistical methods
The SPSS 13.0 statistic software was used for data management. All counting materials were expressed with (). The pairedt-test was used for comparison within the groups. Thet-test of independent samples was adopted for comparison between the groups. Chi-square test was used for the comparison of the counting materials between the groups.P<0.05 was used to represent statistical significance in differences. TheRiditanalysis was used for comparison of the therapeutic effects. The assessment was accomplished independently by special members formally trained and not attending the clinical grouping and treatment.
3.2 Observed indexes
3.2.1 Japanese Orthopedic Association (JOA) scores[4]
The scores were assessed by the therapeutic effects of low back pain from JOA respectively before treatment, and after the 1st, 2nd, 3rd, and 4th course. In the total JOA scores, the highest is 29 points and the lowest is 0 point. The lower the scores are, the more obvious the dysfunction is.
Improvement rate = (Score after treatment - Score before treatment) ÷ (29 - Score before treatment) × 100%.
The improvement rate ≥75% is excellence; the improvement rate ≥50% but <75% is good; the improvement rate ≥30%, but <50% is medium; the improvement rate <30% is poor.
3.2.2 Pain scores
Visual analogue scale (VAS) supervised by Chinese Medical Association was used. A long line segment in 10 cm is printed on the card, with a movable cursor on it. ‘0’ point on the line segment means no pain, and ‘10’point means the severest pain. The patient was told to move the cursor to the corresponding position to record the score depending upon pain situation. Before and after each treatment, the scores were measured and recorded. The scores were assessed before the treatment and after the 1st, 2nd, 3rd and 4th treatment.
3.3 Criteria of therapeutic effects
The diagnostic criteria of lumbar intervertebral disc herniation in the Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[2]were referenced.
Cure: Pain in the low back and thigh disappear, with the straight leg raised over 70°, and the patient is able to restore the original work.
Improvement: Pain in the low back and thigh is relieved and the lumbar movement is improved.
Failure: No change in the symptoms and signs.
3.4 Therapeutic results
3.4.1 Comparison of therapeutic effects between the two groups
In the comparison of the total effective rate after the treatment of four weeks, the differences were statistically significant (P<0.05), indicating that the therapeutic effect was better in the treatment group than in the control group (table 1).
3.4.2 Comparison of JOA scores between the two groups
Before the treatment, there was no statistical difference in JOA scores between the two groups (P>0.05). After the treatment for two courses, JOA scores in the patients of the two groups were obviously elevated than those of the same group before the treatment (P<0.05). After the second course, JOA scores were statistically different between the two groups (P<0.05), (table 2).
3.4.3 Comparison of VAS scores between the two groups
Before the treatment, there was no statistical difference in VAS scores between the two groups (P>0.05). After treatment, VAS scores were obviously decreased in the two groups (table 3).
3.5 Adverse reaction
No adverse reaction occurred in the patient of two groups during the treatment.

Table 1. Comparison of therapeutic effects between the two groups (case)
Table 2. Comparison of JOA scores between the two groups (, point)

Table 2. Comparison of JOA scores between the two groups (, point)
Note: Compared to the same group before the treatment, 1)P<0.05; compared to the control group at the same phase, 2)P<0.05
Treatment 35 10.09±2.13 11.39±2.30 14.24±1.491)2)15.93±3.411)2)21.54±3.411)2)After the 3rd course After the 4th course Control 35 10.36±1.80 10.98±1.81 11.28±1.541)12.02±1.211)18.92±2.891)
Table 3. Comparison of VAS scores between the two groups (, point)

Table 3. Comparison of VAS scores between the two groups (, point)
Note: Compared to the same group before the treatment, 1)P<0.05; compared to the control group at the same phase, 2)P<0.05
GroupsnBefore After 1st course After 2nd course After 3rd course After 4th course Treatment 35 8.362±0.529 7.768±0.675 6.107±2.8221)2)4.981±0.9771)2)2.329±0.9791)2)Control 35 8.277±0.477 7.870±0.539 8.090±2.3451)6.543±0.8211)4.762±0.8661)
4 Discussion
LIDH refers to the lesions mainly characterized by symptoms of pain and numbness in the low back and thigh, caused by partial or complete rupture of the fibrous ring due to external force, single and joint protrusion of the nucleus pulposus and cartilage endplates, irritating or compressing the sinuovertebral nerve and nerve root, after the degenerative change of the lumbar intervertebral disc. The normal disc is elastic and tough, with powerful anti-compressive capability. But, with the increase of the age, degeneration can easily occur in the intervertebral disc. It is commonly believed that the degeneration starts after the age of 20[1]. Due to lack of blood supply and poor repair ability in the intervertebral disc tissue, and at the same time the waist is the axis of the human activity, in a large range, the intervertebral disc bears lots of compression and torsion, so strain is severe. By traumatic injury or infection of pathogenic wind, cold and dampness, rupture can easily happen in the fibrous ring of the lumbar intervertebral disc, leading to protrusion of the nucleus pulposus from rupture, to irritate or compress the adjacent nerve roots and spinal cord, and hence resulting in congestion, edema, degeneration, adhesion and spasm in the surroundingtissues, so as to cause the symptoms of pain in the low back, pain and numbness in the lower limb on one side or two sides. LIDH belongs to the scope of low back pain, Bi-Impediment syndrome of lumbar region, and pain in the low back and thigh in traditional Chinese medicine. Deficiency in the liver and kidney and invasion of exogenous pathogenic wind, cold and dampness are the fundamental factors of this disease, and the external force (except for sudden violent force) is only the inducing factor. Therefore, to reinforce the liver and kidney, nourish the tendons and bones, dissipate pathogenic factors and remove dampness, soothe the tendons and dredge the meridians, circulate qi and activate blood is the major therapeutic method for lumbar intervertebral disc herniation.
Acupoint sticking therapy is a method combined with acupuncture and herbal treatment based upon the theory of meridians in traditional Chinese medicine. In accordance with different diseases and pattern, corresponding herbal stuffs would be selected to make into the plaster and apply to the corresponding acupoints, so as to dredge the meridians and regulate the functions of Zang-fu organs by the irritating effects of herbal stuffs to the acupoints for the prevention and treatment of diseases. As one of the special theories in traditional Chinese medicine and also a new and quickly-developed subject in the modern times, acupoint sticking therapy is effective in the therapeutic effect, without injury and without pain, and without any damage to the spleen and stomach, by direct irritation of herbal stuffs to the acupoints and absorption through the skin, and at the same time the functions are direct because the concentration of herbal stuffs in the local areas are obviously higher than other areas. The remarkable effects could often be achieved in the treatment of many intractable diseases.
The external therapy has been always emphasized to treat the internal diseases in traditional Chinese medicine. Guided by Chinese medical philosophy, and in accordance with the characteristics of herbal stuffs in nature, flavor and attribution to the meridians, proper herbal drugs are selected and manufactured together with the advanced trans-dermal technology into the plaster for acupoint-sticking therapy in this study[5], among which,Yan Hu Suo(Rhizoma Corydalis),Chuan Xiong(Rhizoma Chuanxiong),Dang Gui(Radix Angelicae Sinensis),Dan Shen(Radix Salviae Miltiorrhizae) andHong Hua(Flos Carthami) are supposed to circulate qi, activate blood and stop pain;Mu Gua(Fructus Chaenomelis),Du Huo(Radix Angelicae Pubescentis) andTou Gu Cao(Herba Speranskia Tuberculata) are supposed to soothe the tendons and dredge the meridians;Mo Yao(Myrrha),Chuan Wu(Radix Aconiti) andTian Nan Xing(Rhizoma Arisaematis) are supposed to diminish swelling, circulate qi, activate blood and stop pain;QinJiao(Radix Gentianae Macrophyllae),Xiang Fu(Rhizoma Cyperi),Di Long(Lumbricus) andChuan Niu Xi(Radix Cyathulae) are supposed to expel wind, remove dampness, activate blood and dredge the meridians;Huang Qi(Radix Astragali) is supposed to reinforce qi, produce muscle and promote early elimination of the lesions.Bo He Bing(Mentholum) is able to guide the herbal drugs to reach the diseased area due to its slight cold in nature and its fragrance and constant migration. By transdermal absorption of the herbal stuffs, the plaster applied to Shenshu (BL 23), Yaoyangguan (GV 3), Chengshan (BL 57), Yanglingquan (GB 34) and Ashi points can tonify the liver and kidney, activate blood and expel blood stasis, diminish swelling and stop pain for dealing with both symptoms and causative factors[6-8].
Tuina therapy can be used to relax the tension and muscular spasm in the area with LIDH, can regulate the relative position of the protruded disc and compressed nerve roots, and can also correct the possible complicated dislocation of small joints and is a commonly used conservative therapy for LIDH[9]. The relevant studies showed that the clinical effects are better in the treatment of LIDH by combination of acupuncture and tuina than by single acupuncture or tuina[10].
The results in this study indicate that therapeutic effects and improvement of JOA and VAS scores are better in the treatment of LIDH by external application of herbal drugs than by tuina treatment. The reason to cause difference in the therapeutic effects between the two and if the therapeutic effects by the combined application of external application of herbal drugs and tuina therapy are better than those by single application of two therapeutic methods need to be further studied.
[1] Hu YG. Lumbar Intervertebral Disc Herniation. 3rd Edition. Beijing: People’s Medical Publishing Press, 2004: 107.
[2] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 186.
[3] Luo CG. Science of Tuina. Shanghai: Shanghai Science and Technology Publishing House, 2008: 106-108.
[4] Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Wada E, Yonenobu K, Tanaka T, Hirota Y. JOA back pain evaluation questionnaire: initial report. J Orthop Sci, 2007, 12(5): 443-450.
[5] Zheng ZJ, Xia YY, Chen TX, Cheng LH. Observations on the therapeutic effect of acupoint application on lumbar intervertebral disc herniation. Shanghai Zhenjiu Zazhi, 2011, 4 (30): 246-247.
[6] Huang QF, Wu YC. Exploration of the clinical rule of acupuncture-moxibustion treatment for lumbar intervertebral disc herniation. J Acupunct Tuina Sci, 2009, 7(3): 177-180.
[7] Tao SP, Luo YB, Tang XY, Zhou LY, Song YH, Duan XD, Ding JL. Therapeutic study on acupuncture plus Chinese medicine iontophoresis for lumbar intervertebral disc herniation. Shanghai Zhenjiu Zazhi, 2012, 31(9): 664-666.
[8] Wang BY, Chen TT. Treatment of 40 cases of lumbar intervertebral disc herniation by warm application of herbal drugs plus acupoint sticking therapy. Zhongguo Zhongyi Jizheng, 2011, 20(9): 1527-1528.
[9] Lei LM. Clinical progress of tuina treatment for lumbar intervertebral disc herniation in recent 10 years. J Acupunct Tuina Sci, 2012, 10(2): 128-132.
[10] Huang WS. Observation on the efficacy of combined use of abdominal acupuncture, traction and massotherapy in treating lumbar intervebral disc protrusion. Shanghai Zhenjiu Zazhi, 2008, 27(6): 23-24.
Translator: Huang Guo-qi
R244.1
A
Date: February 20, 2013
Author: Zheng Zhao-jian, deputy chief physician.
E-mail: zhzj1014@163.com
 Journal of Acupuncture and Tuina Science2013年4期
Journal of Acupuncture and Tuina Science2013年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Efficacy Observation on Acupuncture Combined with Auricular Point Sticking Treatment for Primary Dysmenorrhea
- Immediate Effects of Hegu Needling on Adhesive Scapulohumeral Periarthritis
- Clinical Study on Acupoint Injection for Primary Osteoporosis
- Effect of Electroacupuncture on Anxiety and Craving in Heroin Addicts During Detoxification
- Clinical Observation on Electroacupuncture for Post-stroke Flaccid Paralysis
- Treatment of Post-stroke Spastic Hemiplegia by Acupuncture plus Rehabilitation Training