
Think muscle; Think rhabdomyolysis
2018-11-19 07:25:34FatimahLateefArunimaGupta
Journal of Acute Disease 2018年5期
Fatimah Lateef , Arunima Gupta
1Department of Emergency Medicine, Singapore General Hospital, Singapore
2Singhealth Duke NUS Institute of Medical Simulation, Singapore
3Dukes-NUS Graduate Medical School and Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Keywords:Rhabdomyolysis Myoglobinuria Acute kidney injury
ABSTRACT Rhabdomyolysis is the breakdown of striated muscle cells resulting in leakage of cell matter into the extra-cellular space. It can present with myalgia, muscle weakness and swelling.Episodes of passing of dark tea-coloured urine have also been reported. Raised creatinine kinase is diagnostic of rhabdomyolysis. Raised serum myoglobin levels and presence of myoglobin in the urine (myoglobinuria) help to support the diagnosis. The aetiology for rhabdomyolysis can be both traumatic and non-traumatic. In the case of trauma, individuals with crush injuries trapped in cars or under collapsed buildings??, struggling against restraints,immobilized and in the same position for hours due to injuries, comatosed states or positioning during prolonged surgeries and those with high voltage electrical injuries are at increased risk of rhabdomyolysis. Non-traumatic causes of rhabdomyolysis include hyperthermia, metabolic myopathies, drugs and toxins ingestions, electrolyte abnormalities and infections. The mechanism of rhabdomyolysis is often multifactorial. In the case of trauma, direct injury to cell membranes as well as hypoxia from direct compression leading to adenosine triphosphate depletion leads to breakdown of striated muscle cells.. The lysed cells release myoglobin,creatine kinase, urate and phosphate into the interstitium. Direct heme protein-induced toxicity on nephrons can result in acute kidney injury. We report a case of traumatic rhabdomyolysis and share the latest in the literature on the understanding of the subject as well as that of myoglobinuria, with which it is often associated with.
1. Case report
M was a 21 year old man who presented after a fall from a 1 m tall stool that he was using to reach a shelf that was about 2 m in height.The stool gave way and he landed on his back with the proximal aspect of his right leg being caught in between the legs of the stool,with some degree of twisting, bringing the knee joint into a varus position. His head hit the marble slab behind him.
He experienced a tremendous amount of pain, did not have any loss of consciousness, dizziness or headache. He had no jerking movements, urinary or bowel incontinence or tongue-biting,suggestive of a seizure. The maximum pain was along the anterior-lateral aspect of his right leg and there was a muscle spasm in that area. There was no pain radiation reported. He described the pain as severe and squeezing in nature, with a pain score of 8/10. This pain was associated with numbness on the anterior aspect of the right thigh. He did not report any “pop” sound when his knee was twisted.Prior to the fall, M did not experience any chest pain or palpitations.He did not have any dizziness. He had not consumed any alcohol or drugs.
M had no significant past medical history and was not on any chronic medications, supplements or traditional Chinese medications.He exercises 6 days a week and each session is approximately 2 hours. He also consumes protein powder shakes twice a week. His last exercise session was the morning of the incident, approximately 8 h before the incident.
On examination, M’s vitals were stable. His temperature was 36.9 ℃ Blood pressure was 123/73 mmHg, Heart rate was 90 beats per minute and respiratory rate was 14 breathes per minute.His ECG showed sinus tachycardia. Glasgow Coma Scale was full(15/15) with pupils reactive to light. He appeared well but in pain.His overall physique was very muscular and well built. The muscles over his anterior right thigh were tense with visible spasms. The range of motion was significantly inhibited by pain. There was no tenderness along the joint line of the knee and no effusion. Anterior and posterior drawer tests were negative. Reflexes were present and normal. The right hip flexion and extension was 3/5 (inhibited by pain), and ankle flexion and extension was 4/5. Straight leg raise test was negative. Capillary refill time of his big toe was under 2 seconds. The left lower limb was normal. Examination of the cranial nerves and upper limbs were also normal.
Heart sounds were normal and his lungs were clear. The abdomen was soft and non-tender. His calves were supple. There was no step deformity or tenderness in the spine and no hematoma over the back. Perianal sensation and anal tone was intact on digital rectal examination. M was able to demonstrate walking a short distance of 2 m on the emergency department, limited by the pain in his thigh.Blood investigations included serum creatinine kinase (CK) and myoglobin levels, renal panel, liver function test, coagulation profile and a full blood count. The results are shown in Table 1. X rays of lumbar spine and right femur were normal.
He was given pain relief using the combination of tramadol,morphine and paracetamol in view of his significant pain. In light of the muscle spasms and raised CK as well as myoglobin, M was given intensive hydration both orally and intravenously. In the ward his enzymes levels were trended and pain control optimised and after 3 days he was discharged, with a follow up in 2 weeks at the Specialist Outpatient Clinic. He was diagnosed to have rhabdomyolysis secondary to a trauma from a mechanical fall complicated by paininduced right lower limb weakness.
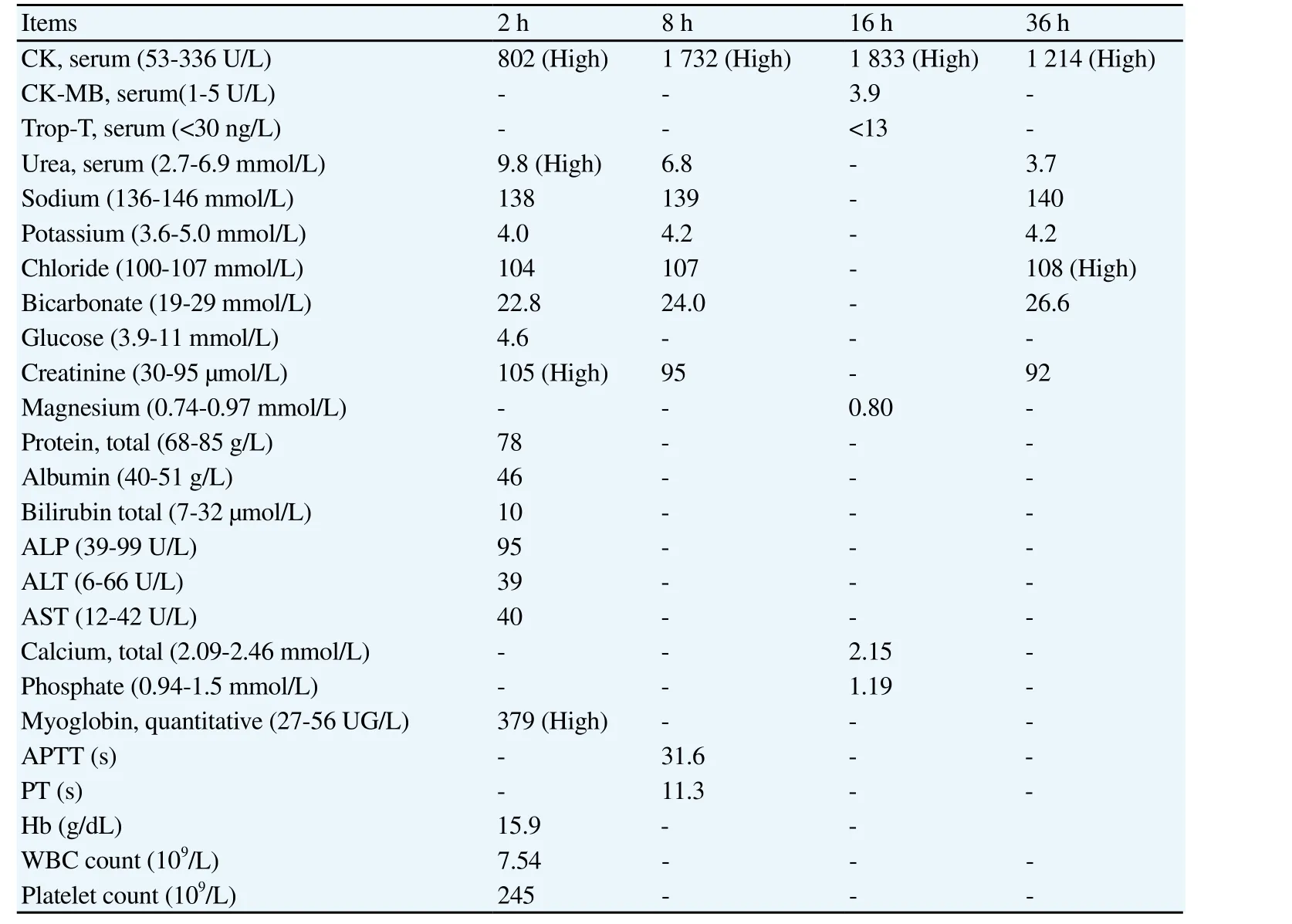
Table 1 Results trend for patient M over the course of hospitalisation (values in brackets reflect the normal laboratory range).
2. Discussion
Rhabdomyolysis is a complex and potentially life threatening syndrome which is characterised by the breakdown of traumatised skeletal muscle fibres. This in turn leads to the release of intracellular components such as myoglobin, CK, aldolase, lactate dehydrogenase and other electrolytes. Any minimal damage can initiate the process of rhabdomyolysis. The presentation can be a spectrum, from being asymptomatic at very low levels to more serious presentation with the higher levels of CK, significant electrolyte disturbances and even acute renal failure and disseminated intravascular coagulation[1-4].
Traumatic causes seem to be more often and easily diagnosed,but rhabdomyolysis can also happen in atraumatic cases, such as those related to drug ingestion, metabolic problems, serious and often extensive infections, toxins and poisoning cases and some genetic diseases, which predisposes to its development. There have even been documented cases of rhabdomyolysis requiring renal transplant. Traumatic cases prone to rhabdomyolysis includes severe injuries such as bombings, blast injuries, building collapse during earthquakes, high voltage electrical injuries and others Serum CK levels do rise naturally after strenuous exercise in most individuals and this is also something to bear in mind[5,6].
Some patients have been seen to present with a triad: myalgia,weakness and myoglobinuria. However it was observed that less than 10% of patients have the triad. In fact more than 50% of patients affected by rhabdomyolysis do not have weakness as a presentation[7,8].
Patients may present with a whole spectrum of muscle pain; from myalgia (pain only) to myositis (pain associated with elevated CK levels) to the more serious rhabdomyolysis (where some have suggested that the CK levels are raised, usually more than 11 times normal and associated with myoglobinuria or tea coloured urine).Elevation of plasma CK is the most sensitive laboratory test related to muscle injury[8,9]. In our patient his highest CK level was 1 833 U/L (530336) at 36 h post fall. Subsequently, the levels downtrended.The highest documented CK level in the literature search was a 7 –digit CK rise in a child. The level was 1 778 856 U/L (normal range 20-200 U/L). This was in a child with lipin-1 mutation that causes recurrent rhabdomyolysis in children. This gene encodes the muscle specific phosphatidic acid phosphatase, an enzyme critical in phospholipid biosynthesis[10,11].
What is unique with our patient, M, is that his trauma was relatively low impact compared to the usual types of trauma which lead to rhabdomyolysis. There was also no significant description of crushing, crush injury or prolonged extrication. Regardless, it still led to considerable rhabdomyolysis. Perhaps his exercise regime may have had some contribution to his CK levels.
In a paediatric patient, a patient with chronic, progressive neuromuscular symptoms or a patient with recurrent rhabdomyolysis, metabolic errors such as metabolic myopathies should be considered. As there is no baseline to compare to in our case, it is still important to assess whether or not the patient has some underlying pathology causing raised baseline CK and myoglobin levels[10,11]. In particular this patient was very muscular and he was serious with his exercise and muscle building. He did this 6 times a week and also took protein drink supplements. Strenuous exercises performed under hot and humid conditions have been known to cause severe rhabdomyolysis but he did not have such an exposure.Possible metabolic myopathies, electrolyte disorders or consumption of illicit drugs can also be considered as they may have led to a subclinical non-traumatic rhabdomyolysis prior to the fall. Should the patient’s serum creatinine kinase have been elevated on follow up, further workup to exclude these underlying pathologies will be crucial. However at 2 weeks follow up after discharge there levels had returned to normal and he was well.
This patient also had an MRI of his lumbar spine done as he had landed on his back and the pain in the right femur was significant.The MRI study was normal.
A key lesson from this case is the importance of adequate hydration as soon as possible in a patient suspected to have rhabdomyolysis.Hypovolemia and dehydration are known pre-disposing factors for the nephrotoxic effects on myoglobin[12,13]. In the case of M,fluid therapy was key in preventing acute kidney injury (AKI) from occurring which would have prolonged hospital stay and could have had long term consequences. Early and vigorous fluid therapy can help alleviate hypovolemia and correct electrolyte imbalances[14].
As intravascular volume increases, renal blood flow increases and there is greater excretion of nephrotoxic compounds which can potentially causing AKI. It is also reported that an acidic environment promotes myoglobin toxicity and hence Ⅳsodium bicarbonate can also be given to minimise the nephrotoxicity. However, there is no proven benefit as no studies have been done comparing a combined study to Ⅳfluid therapy[12-14].
When managing patients with rhabdomyolysis, it is important to be aware of the potential complications that can occur and to anticipate them in advance. This will help make the outcomes better for our patients[15-19].
1) Hypovolemia: this is the commonest by far as the sequestration of fluid into the traumatised muscles can be significant. The muscles will become ‘edematous’. The treatment for this is to ensure adequate fluid regime and replacement;
2) Hypocalcaemia: this is due to the inward flux of, binding phosphatidyl inositol. The immediate response might be to replace calcium but this is not recommended because of point 3 below;
3) Hypercalcaemia: this tends to follow the initial hypocalcaemia phase but the time of onset if variable and depends on how extensive the muscle damage and trauma is. The damaged muscles release calcium and in turn the may be slowed down due to the development of AKI in some patients. The best treatment for this ios adequate hydration and customised diuresis, with strict input and output monitoring;
4) Hyperkalemia: this is released from the traumatised and damaged muscle cells and the usual treatment for hyperkalemia should be instituted i.e. calcium gluconate infusion, insulin-dextrose regime and sodium bicarbonate infusion;
5) Hyperphosphataemia: this is also from muscle breakdown and the best treatment is hydration and customised diuresis. In severe cases,haemodialysis may be indicated;
6) DIVC: this happens due to the thromboplastin release and thromboplastic microangiopathy can become widespread is those with large amounts of muscle damaged
7) Compartment syndrome: due to the edema of the muscles and the continued sequestration as well as the associated bleeding in the area are all contributory. Thus the importance of monitoring distal neurovascular status and pain in affected limbs
8) AKI: this has abrupt onset, usually within 1-7 d and is usually sustained more than 24 h, with a reduction in renal function. There is the RIFLE (Risk, Injury, Failure, Loss and End stage) (2004) or the AKIN (AKI Network) (2007) criteria, which can both be used to objectively define the degree and severity of AKI.
3. Conclusion
Rhabdomyolysis is a possible complication of trauma and may be subclinical. A high index of suspicion is important. If one does not think about this, one may miss making the diagnosis. It is an important consideration in patients in the emergency department who present with trauma, even if the level of trauma does not satisfy the expected intensity and impact. Investigations should be done as soon as possible to confirm the diagnosis of rhabdomyolysis and IV fluid therapy should be started immediately upon diagnosis. This can help reduce the progression to significant AKI and minimise further complications
Conflict of interest statement
The authors decclare that we have no conflict of interest.
 Journal of Acute Disease2018年5期
Journal of Acute Disease2018年5期
- Journal of Acute Disease的其它文章
- CORRIGENDUM
- False negative diffusion weighted imaging in an acute onset double vision patient with isolated internuclear ophthalmoplegia from ischemic origin
- A case of human acute otoacariasis caused by Rhizoglyphus sp, the first report from Iran
- Intracranial hematoma development following thrombolysis inpatients suffering with acute myocardial infarction: Management strategy
- Survival rate among tuberculosis patients identified in south of Iran,2005-2016
- Inhibiting effect of immunoeffector cells induced by denderitic cells vaccine on growth of PC3 and BEL7402