
Rheumatoid arthritis accompanied by discoid lupus erythematosus
2019-04-03 02:13:58LingLingZhangZhuoChenDavidMubangaXinLingBiYuLingShi
國際皮膚性病學(xué)雜志 2019年1期
Ling-Ling Zhang,Zhuo Chen,David Mubanga,Xin-Ling Bi*,Yu-Ling Shi*
1Deptment of Dermatology,Changhai Hospital,Second Military Medical University,Shanghai 200433,China.2Department of Dermatology,Shanghai Children’s Medical Center Affiliated to Shanghai Jiao Tong University School of Medicine,Shanghai 200127,China.3Department of Dermatology,Shanghai Tenth People’s Hospital,Tongji University School of Medicine,Shanghai 200072,China.
Introduction
Subacute cutaneous lupus erythematosus(SCLE),discoid lupus erythematosus(DLE),and systemic lupus erythematosus(SLE)are three of the distinctive subsets of lupus erythematosus(LE).Peter Schur,in 1971,coined the term“rhupus”to describe the patients satisfying the criteria of both SLE and rheumatoid arthritis(RA)[1].In 2013,the globally cumulative number of rhupus cases reported was about 140[2].RA combined with SCLE has also been reported,while the RA with DLE has never been described.Herein,we report a case of RA,who developed DLE after 10 years of RA.
Case report
In June 2017,a 55-year-old man developed a pink patch on the scalp.A few weeks later,similar lesions appeared on his forehead,nose,temporal region,and forearms(Figure 1A).The patient had a 25-year history of RA that had resulted in severe joint damage of the hands and knees.At the time of presentation,
the patient was taking 50 mg of diclofenac sodium twice daily and 4 mg of methylprednisolone once daily for his RA.He had been taking the diclofenac sodium for approximately 10 years.He denied a history of oral ulcers,alopecia,chest pain,pleurisy,or sicca complex.The patient did not seek medical attention at the time due to his poor social economic status.In early December 2017,the patient visited a rheumatologist for knee joint pain.The doctor prescribed weekly treatment with 10 mg of methotrexate and advised him to consult a dermatologist for the skin lesion.
Due to a lack of DLE lesion improvement,the patient visited a dermatology clinic two weeks later.Upon examination,the patient showed severe RA with bilateral ulnar deviation and destructive changes in all fingers along with swelling in both wrists and in the left knee(Figure 1B).Radiographic examination revealed significant destruction of joints,including carpus,metacarpophalangeal joints,and interphalangeal joints.
Examination of the skin revealed pink patches on the head,nose,temporal region,and extensor surface of the forearms.Skin biopsy followed by a histological examination of the lesion revealed a marked atrophy of the epidermis and liquefaction degeneration of the basal cell layer.Capillary proliferation along with lymphocyte and histiocyte infiltration in the superficial dermis and around the blood vessels of appendages were also observed(Figure 2A and 2B).Results of serological examination were as follows:antinuclear antibody(ANA):positive(homogeneous);immunoglobulin(Ig)G:19.30 g/L (normal range:7.51-15.6 g/L);positive rheumatoid factor:titer of 1:2,410IU/ml(normallevel:< 20IU/ml);antistreptolysin(ASO)antibody:143IU/ml(normal level:<116 IU/ml);anti-cyclic citrullinated peptide antibody:47.40 RU/ml(normal level:<25 Ru/ml);and erythrocyte sedimentation rate(ESR):66 mm/h(normal level:<15 mm/h).The results of anti-native DNA assays were negative or normal.Tests for antibodies against Ro(SS-A)or La(SS-B)also produced negative results.
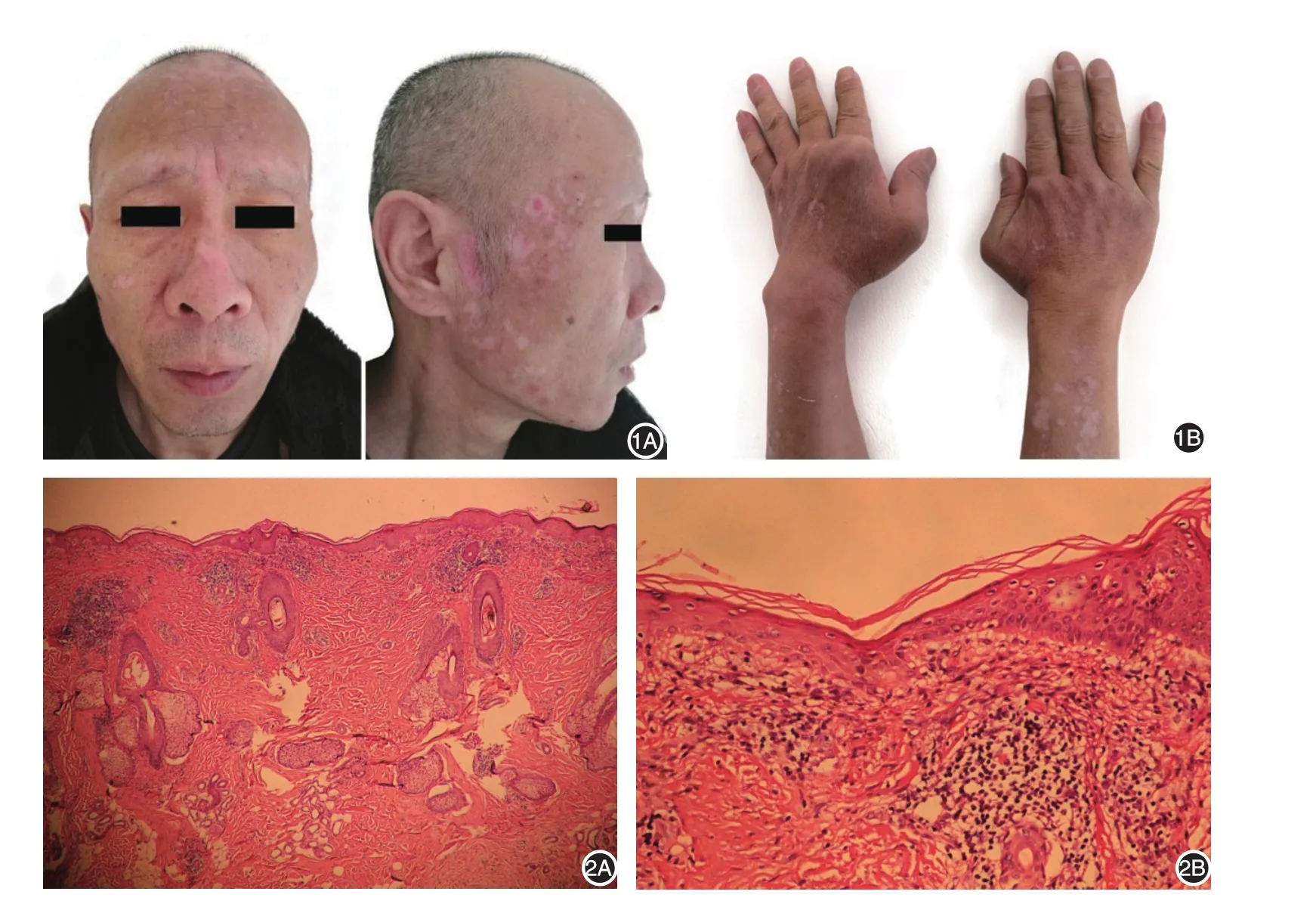
Figure 1 Skin DLE lesions and RA manifestations.A:Pink patches on the scalp,forehead,nose,and temples.B:Bilateral ulnar deviation with destructive changes in all fingers and swelling in both wrists.Figure 2 Histological manifestations of the patient’s DLE lesions.A:Capillary proliferation with lymphocyte and histiocyte infiltration in the superficial dermis and around the blood vessels in the appendages(H&E,×100).B:Atrophy of the epidermis and liquefaction degeneration of the basal cell layer(H&E,×400).
The patient was subsequently treated with 100 mg of hydroxychloroquine sulfate twice daily along with topical clobetasol propionate.He gradually got better within one month.As of the time of writing,the patient is still being followed up.
Discussion
Hereditary predisposition,viral infection,drugs,ultraviolet radiation,and gonadal hormones are all thought to be related to LE.Single or multiple,round or oval,sharply demarcated,rose-pink lesions accompanied by adherent scaling and follicular dilation typically appear on sun-exposed sites.These lesions tend to appear most often on the face,scalp,and auricular regions,and the eruptions are often aggravated by sun exposure.DLE in particular is closely related to sun exposure.One report indicates that 1.3%-5.0%of DLE may develop into SLE[3],whereas another suggests that up to 17%of DLE may develop into SLE[4].Furthermore,15%of SLE patients have DLE skin lesions.
There are many reports about RA combined with LE.The coexistence of RA with SLE is known as rhupus syndrome,the prevalence of which is 0.09%[5].Previous work showed that rhupus patients have milder SLE activity and a lower incidence of visceral organ involvement compared with SLE patients without RA[6-7].The exact etiology and triggers of rhupus remains unknown till date.There are also several reports of RA combined with SCLE[8-9].Migitaet al.[6]reported a case of RA with Sj?gren’s syndrome(SS)in which the patient developed SCLE;serological tests showed that the patient’s anti-SS-A/Ro antibody and anti-DNA antibody levels were elevated.Additionally,Pantojaet al.[9]reported the case of a 51-year-old woman with RA who developed anti-La/SSB antibodies and erythematosquamous lesions on her upper back;the histological diagnosis was SCLE.
Our patient presented multiple unusual clinical features.First,his DLE occurred after a 25-year history of RA.The patient had no history of extensive sun exposure prior to the appearance of the eruption,and his laboratory evaluation results were unremarkable,except for a positive ANA(homogeneous)finding.Based on these initial findings,a diagnosis of DLE without associated systemic disease was made.Two weeks later,a rheumatologist prescribed methotrexate to the patient,but this treatment failed to improve his DLE lesions.However,the patient improved after he was treated with hydroxychloroquine sulfate and topical clobetasol propionate.Notably,the patient’s lesions were disseminated,so he has an increased risk of his condition developing into SLE;thus,further follow-up of this patient is necessary.
Acknowledgement
This work was supported by Chinese Society Dermatology Bright Future foundation.
- 國際皮膚性病學(xué)雜志的其它文章
- Paraneoplastic pemphigus comorbid with cardiac cancer and duodenal gastrointestinal stromal tumors:a rare case report
- Reactive perforating collagenosis
- Sun?protection knowledge and strategies of Chinese dermatologists:a nation?wide,questionnaire?based survey
- Initial presentation of acute myeloid leukemia in a patient with cutaneous myeloid sarcoma
- Persistent papules with adult?onset Still’s disease:a case report
- Primary vulvar melanoma in a 27?year?old pregnant woman:a case report and literature review