
Ureter - an unusual site of breast cancer metastasis:A case report
2019-04-18 07:23:22ZhongHanZhouLiJiangSunGuiMingZhang
World Journal of Clinical Cases 2019年20期
Zhong-Han Zhou,Li-Jiang Sun,Gui-Ming Zhang
Zhong-Han Zhou,Li-Jiang Sun,Gui-Ming Zhang,Department of Urology,The Affiliated Hospital of Qingdao University,Qingdao 266003,Shandong Province,China
Abstract
Key words:Breast cancer;Ureter metastasis;Immunohistochemistry;Chemotherapy;Case report
INTRODUCTION
Breast cancer(BCa)is one of the most common malignancies in women,with over 1.5 million new cases diagnosed annually worldwide[1,2].Approximately 12% of BCa patients develop metastatic disease after surgery,with the most common metastatic sites being the bone,liver,brain,spinal cord,and lungs.Other sites of metastatic BCa colonization include the stomach,spleen,ovary,uterus,pituitary,and kidney[3].Ureteral metastasis from non-urinary system tumors,such as BCa,has rarely been reported[4].Herein,we present a case of pathologically confirmed ureteral metastases of BCa,providing clinical experience for its diagnosis and treatment.
CASE PRESENTATION
Chief complaints
A 55-year-old Chinese woman was admitted to the Department of Urology of The Affiliated Hospital of Qingdao University,complaining of lower back pain for 3 mo.
History of present illness
The patient’s symptoms started 3 mo ago with lower back pain.She reported no obvious gross hematuria.
History of past illness
Eight years prior,the patient was diagnosed with BCa and underwent left modified radical mastectomy.Histopathological results revealed infiltrating ductal carcinoma and axillary lymph node metastasis(12/15).Immunohistochemical examination revealed the following characteristics:estrogen receptor(ER)(2+),progestin receptor(PR)(3+),and HER2(-).The tumor was defined as T2N2M0,and the patient received four cycles of the EC protocol [epirubicin:180 mg/m3(d1),70 mg/m3(d2),cyclophosphamide:800 mg/m3(d1)] and four cycles of the T protocol(docetaxel:75 mg/m3),followed by radiotherapy(50 Gy;25×).Then,the patient began to take toremifene citrate tablets(60 mg qd)and regularly revisited the hospital.Four years ago,she received subclavian and submandibular clearance when palpable masses were found on physical examination.Immunohistochemical results demonstrated that these masses were BCa metastases:ER(2+),PR(1+),HER2(0),and P53(3+),which were treated with six cycles of the DP protocol [docetaxel:120 mg/m3(d1),cisplatin:60 mg/m3(d1-2)] and radiotherapy(50 Gy;20×).Then,one year ago,once again a mass was found in her right breast.She underwent right modified radical mastectomy and axillary lymph node dissection.Immunohistochemistry showed:ER(2+)and PR(2+),and she received another round of the EC and T protocols.Three months ago,she felt a mild lower back pain.A positron-emission tomography/computed tomography scan indicated progression of the axillary lymph node metastases,so the patient received targeted therapy(apatinib,500 mg qd).After 3 mo of targeted therapy,the patient revisited the hospital for further evaluation.
Personal and family history
The patient had no personal or family history.
Physical examination upon admission
No positive signs were found during physical examination.
Laboratory examinations
Three consecutive urine cytological examinations found no malignant cells on smears.Several tumor markers were elevated:CEA:6.46 ng/mL(normal 0-3.4 ng/mL),CA15-3:38.41 U/mL(normal 0-25 U/mL),CA19-9:105.60 U/mL(normal 0-39 U/mL),and CA125:19.56 U/mL(normal 0.35 U/mL).
Imaging examinations
A computed tomography urography scan reported a severe obstruction in the lower left ureter segment along with left hydronephrosis(Figure 1).

Figure 1 Computed tomography urography scan showed a severe obstruction in the lower segment of the left ureter along with left hydronephrosis.
FINAL DIAGNOSIS
The final diagnosis of the present case was ureteral urothelial carcinoma.
TREATMENT
Upon admission,we first performed an ureteroscopy,and observed a stenosis(approximately 1.5 cm)that was approximately 3 cm in length from the left ureteral orifice.The wall was thick and stiff,without cauliflower-like or corpora mammillaria neoplasms,thus we did not take a biopsy.One week later,the patient underwent a laparoscopic exploratory laparotomy.During the operation,a ureteral lesion was resected for frozen histopathology,which showed that the muscular layer and tunica adventitia of the ureter were infiltrated by poorly-differentiated cancer cells.Then,a laparoscopic nephroureterectomy was performed,removing out the whole kidney and ureter.Histopathological evaluation of the resected specimen revealed that the muscular layer and tunica adventitia of the left ureter were locally infiltrated(4 mm in diameter under the microscope),without infiltration into the mucous layer of the ureter(Figure 2).There were no malignant tumors in the kidney pelvis or parenchyma.Infiltration was also found within the fibrous and adipose tissue around the porta renis(4 mm in diameter under the microscope).Immunohistochemical examination revealed the following:ER(weakly +,10%)(Figure 3A),PR(-)(Figure 3B),HER2(1+),Ki-67(30%),E-Cad(+),P120(+),GATA3(+),GCDFP-15(-),Mammaglobin(-),and P63(-).Based on her medical history and these histopathological findings,the postoperative diagnosis of ureteral metastases from BCa was confirmed.
OUTCOME AND FOLLOW-UP
The patient had an uneventful postoperative clinical course and was discharged from hospital 6 d after the operation.As suggested by her oncologist,she continued to receive apatinib.Postoperative 3-mo follow-up indicated progression of the axillary lymph node metastases.
DISCUSSION
First reported in 1909,ureteral metastasis of any prior tumor is extremely rare[4,6].In 1999,a total of 342 cases of ureteral metastases were collected and reviewed by Haddadet al[4].Stomach,prostate,and bladder cancers are the most common primary malignancies to develop ureteral metastases,and BCa accounts for 7.8% of all cases[4,6].Only a few new cases have been reported over the past 18 years[7-13].
In this case,the patient complained of a 3-mo history of lower back pain,but had no history of hematuria.Most ureteral metastases are asymptomatic,and only 36% of cases presented nonspecific systemic symptoms such as lumbar pain,nausea,urinarytract infection,or weight loss[4,14],among which,pain due to ureteral obstruction is the most frequent symptom.Hematuria is not commonly seen,because the primary tumor usually metastasizes beneath the mucosa or invades from surrounding tissues[15].
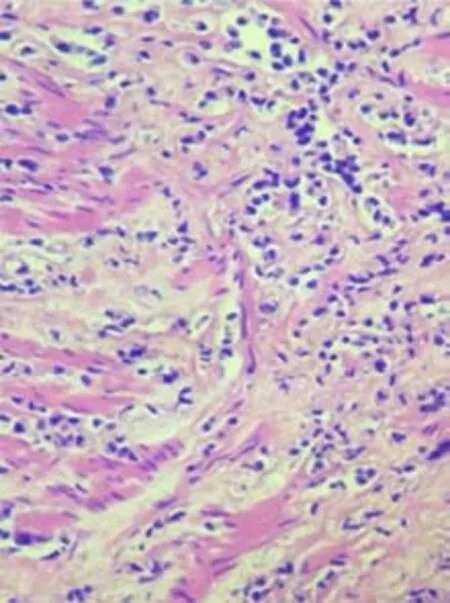
Figure 2 Hematoxylin and eosin-stained histological ureter section showing infiltration of poorly differentiated tumor cells that displayed an alveolar growth pattern(magnification,100×).
It is difficult to distinguish metastatic ureteral tumors from ureteral urothelial carcinoma.Clinical histories may provide hints;however,they are usually insufficient.Metastatic ureteral tumors tend not to adhere to the mucosa;thus,urine cytology offers little help.Presmanet al[16]reported that metastatic ureteral cancers often present with several characteristics:Tumor cells in the lymph nodes and vessels around the ureter,or the same type of cells in the ureteral wall without direct invasion.Biopsy under ureteroscopy may facilitate obtaining a precise diagnosis,but it should be pointed out that because of the limited sample size,pathological diagnoses are sometimes indistinct.In this case,ureteroscopy only observed a stenosis of the ureter without a proper biopsy.Thus,exploratory laparotomy is recommended,and further clinical decisions should be made according to the pathological section when it is difficult to make a clear diagnosis by ureteroscopy.
Currently,there is no cure for metastatic BCa[3].Surgical resection of the primary tumor or isolated metastatic lesions may be an effective therapeutic strategy.Radiotherapy can be performed to target the tumor or postsurgical tumor site[17,18].Systemic treatment is normally added to those treatments and is based on the primary tumor or metastatic sites[19].Chemotherapy is the most commonly used systemic treatment,and alternatives to chemotherapy include hormonal therapy,moleculartargeted therapy,immunotherapy,and recently nanotechnology and gene therapy[20].
The median survival of metastatic patients has been reported to range from 24 to 30 mo with a small percentage of them surviving a few months or a few years.With regard to metastatic site,organ diffusion,especially liver and/or soft tissues,is reported to be a predictor of poor survival[21].In this case,the patient received targeted therapy after the progression of axillary lymph node metastases.Three months later,ureteral metastases from BCa were confirmed.Then,the metastatic lesions were resected,and postoperative 3-mo follow-up indicated further progression of the axillary lymph node metastases,indicating a relatively poor oncological outcome.
CONCLUSION
Herein,we report a rare case of ureteral metastases from BCa.Such a diagnosis is usually established by histopathology and immunohistochemistry.The nonspecific symptoms of this condition add to the difficulties of making the diagnosis.We emphasize the importance of histopathology by ureteroscopy and frozen histopathology during operation when making clinical decisions.
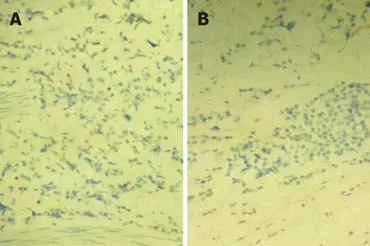
Figure 3 lmmunoreactivity in tumor cells.
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Rh-incompatible hemolytic disease of the newborn in Hefei
- Ureteral Ewing’s sarcoma in an elderly woman:A case report
- Anaplastic lymphoma kinase-negative anaplastic large cell lymphoma masquerading as Behcet's disease:A case report and review of literature
- Synchronous quadruple primary malignancies of the cervix,endometrium,ovary,and stomach in a single patient:A case report and review of literature
- Sister Mary Joseph’s nodule in endometrial carcinoma:A case report
- Alternative technique to save ischemic bowel segment in management of neonatal short bowel syndrome:A case report