
Investigation for the transcultural self-efficacy of nurses in Guizhou,China
2020-06-15 07:37:24JunLiBiWuZhungJiruLiuRongXioYongLuo
Jun Li ,Bi Wu ,Zhung H ,Jiru Liu ,Rong Xio ,Yong Luo
a Guizhou Provincial People’s Hospital,Gui Zhou,China
b Rory Meyers College of Nursing,New York University,New York,USA
c School of Nursing,Guizhou University,Gui Zhou,China
d School of Nursing,Guizhou University of Traditional Chinese Medicine,Gui Zhou,China
e RN,Saint Agnes Hospital,Baltimore,MD,USA
f Chongqing Population and Family Planning Science and Technology Research Institute,Chongqing,China
Keywords:China General hospitals Minority groups Nurses Self efficacy Surveys and questionnaires Transcultural nursing
ABSTRACT Aim:As conflict caused by cultural diversity among patients in China continues to rise,hospitals are in urgent need for improvement of transcultural efficacy among nurses.This study aims to evaluate the transcultural self-efficacy of nurses working in the tertiary general hospital in Guizhou Province,an ethnic minority region in western China,and to identify whether nurses’ demographic characteristics affect their transcultural self-efficacy.Method:We used the Chinese version of the Transcultural Self-Efficacy Tool(TSET-CV)to survey 1,190 inservice nurses.Results:Results showed that the level of transcultural self-efficacy of the nurses was generally moderate;few of the nurses had high or low transcultural self-efficacy.The nurses’ transcultural self-efficacy was affected by demographic variables,including age,marital status,employment type,income,work experience,and whether or not they were head nurses.Having a stable work environment,a stable marriage,a good educational background,and a high-ranked professional title were associated with increased transcultural self-efficacy.Conclusion:Nursing administrators in hospitals should offer continuing education on transcultural nursing according to nurses’ demographic characteristics and the SEST scores.
What is known?
· Transcultural self-efficacy is defined as a nurse's confidence when providing nursing care for patients from different cultural backgrounds.
· A nurse's lack of perceived transcultural self-efficacy will cause patients with cultural differences to feel discriminated against and miscommunicated with which can lead to incorrect diagnoses and invalid nursing interventions.
What is new?
· This study demonstrated that the transcultural self-efficacy level (SEL)of the nurses was generally moderate;few nurses had a high or low transcultural SEL.
· The self-efficacy strength (SEST)scores of the nurses were affected by age,marital status,employment type,professional title,income,work experience in different departments,and job title.
· Nursing management in hospitals should offer continuing education on transcultural nursing according to nurses' demographic characteristics and the SEST scores.
1.Introduction
Societies are becoming increasingly multicultural with plurality of cultures existing withinor between countries [1].Transnational culture is applicable tomulticultural nursing among different countries,ethnic groups and different cultures within a country[2].While the ethnic majority in China is Han Chinese,it is also inhabited by multi-ethnic populations.The relationship between ethnic minorities and the dominant Han Chinese has been explored previously in research studies.The Han Chinese and China’s ethnic minorities have different habits,languages,religions,dietary habits,and values.These specific cultural differences create the unique polymorphic sub-cultural phenomena of Chinese culture[3].
Traditionally,the level of economic development in the eastern coastal areas is much higher than that in the western regions.In the year 2000,Chinese government launched the Western Development Strategy in 12 provinces inhabited by ethnic minorities with the aim to promote economic develop in this region.Guizhou,a province that is currently experiencing an underdeveloped economy,is one of the provinces targeted by the Western Development Strategy that has the characteristics of a polymorphic subculture.The ethnic minority populations live on the plateaus,mountains,and the canyons of the region’s karst landscape.This closed environment preserves a national and traditional cultural heritage that is characterized by the ancient Chinese saying,“Winds are different within 10 miles;customs vary within 3 miles.” Such ethnic minority cultures are rare in China and across the globe [4].Currently,Guizhou Province is home to 49 ethnicities and more than 12.5 million people.It has the third-largest ethnic minority population in China [5].Eighteen of the 49 ethnicities are resident ethnic minorities,accounting for approximately 6 million people.Most of these ethnic minorities have their own spoken and written languages that they use for daily communication[6].Guizhou is also a religiously diverse province.Of the five different religions present in the province (Catholicism,Christianity,Islam,Buddhism,and Taoism),ethnic minorities account for approximately 70% of believers.In addition,folk or traditional religions of the ethnic minority groups also play an important role in the social lives of the resident ethnic minorities.
Due to the Western Development Strategy,massive migration of resident ethnic minorities from rural settlements to cities in Guizhou Province have been underway since 2000.The total number of migrant workers moving from the rural settlements to the cities of Guizhou Province reached 12.98 million people in 2015[7].Ethnic minority migrant workers who migrate to cities dominated by the dominant culture do not only confront economic and social pressures created by the differences between rural and urban areas,but also encounter the difficulties of cultural adaption.This phenomenon has increasingly attracted the attention of scholars in China.As an underdeveloped province in China,Guizhou experience uneven allocation of medical resources,which creates enormous rural-urban disparities.Eighty percent of the existing health care resources in Guizhou Province,including the highest-grade hospitals (i.e.,tertiary general hospitals),are concentrated in large modern cities such as the provincial capital,Guiyang City[8].
Both the Western Development Strategy and the unequal allocation of medical resources in Guizhou Province have promoted the influx of a large number of the native minority patients from rural areas to the general hospitals in the big cities.However,nurses in urban tertiary general hospitals usually receive only a basic nursing education that abide by Han characteristics.Their living and working environments are immersed in urban mainstream culture,and their working language is Mandarin.Leninger states that beliefs,values,expressions,behaviors,and attitudes toward birth,senility,illness,and death are unique in every culture [9].Nurses must interact with a large number of patients from different cultures practicing all of these unique aspects and conflicts arise between ethnic minority,mainstream,subculture,urban,or rural cultures as a result.These multicultural conflicts have posed severe challenges to transcultural nursing competence among nurses in the large cities of Guizhou Province.
Leninger’s theory of cultural differences and similarities suggest that cultural differences exist between different countries and nations.Non-mainstream cultures and subcultures also exist within mainstream cultures[9].Bandura’s perceived self-efficacy theory is the important theoretical basis of this study [10].Bandura’s selfefficacy theory refers to a person’s confidence or belief in their ability to achieve behavioral goals in specific fields.Transcultural self-efficacy is defined as a nurse’s confidence when providing nursing care for patients from different cultural backgrounds [11].Some studies [12-14]have indicated that a nurse’s lack of perceived transcultural self-efficacy will cause patients with cultural differences to feel discriminated against and miscommunicated with which can lead to incorrect diagnoses and invalid nursing interventions.A study showed that nurses’ lack of perceived transcultural self-efficacy can also cause an increased risk of depression and pain in patients [15,16]used Bandura’s model[10]to propose that an individual with a high level of perceived self-efficacy(confidence)will take the initiative to seek knowledge that improves his or her transcultural nursing skills and cultural competence.The improvement of transcultural self-efficacy is vital for nurses,as they face an increasing number of patients of different cultural backgrounds [17].
Meanwhile,doctor-patient conflicts in China are growing more intense,with the incidence of medical disputes escalating [18].Improving hospital nurses’perceived transcultural self-efficacy and skills has become a pressing issue for Chinese nursing management.However,for some time,nursing education in China has been overly focused on basic medical education while neglecting humanity education [19].Providing tailored continuing education according to nurses’demographic characteristics can improve their transcultural self-efficacy and later,transcultural capability[20].No relevant study has previously been conducted in China.The reason being that scholars or studies in China have not proposed continuing education programs for transcultural nursing because no one so far has analyzed the training needs of different nurse groups from an empirical perspective.
The purpose of our study is to assess the current perceived transcultural self-efficacy among nurses in Guizhou and to discuss the demographic characteristics related to nurses’ perceived transcultural self-efficacy.
To that effect,this study aims to(a)assess nurses’perceived selfefficacy level (SEL)and perceived self-efficacy strength (SEST),SEL and SEST are the two dimensions of nurses’perceived self-efficacy,and to(b)discuss demographic characteristics in relation to nurses’perceived transcultural self-efficacy.
2.Method
A cross-sectional survey was conducted among 1,190 nurses working in three tertiary general hospitals in Guizhou Province,China to collect data about the transcultural self-efficacy of relevant personnel.The sampling methods included both quota sampling and convenience sampling.
The nurses who participated in the survey were all volunteers and were informed of the purpose and significance of the study by the research group members.Our study passed the review by the ethics committee at Chongqing Medical University and was approved by the Nursing Department and the Clinical Department at the three participating hospitals.
2.1.Sample
The sample included nurses at three tertiary general hospitals located in the capital of Guizhou Province:Guiyang City.Each hospital has about 2,000 nurses and 2,500 beds.Guiyang is an important modern,multi-ethnic city in southwest China.It is also a center for high quality healthcare resources in Guizhou Province.Hence,Guiyang City is the main destination for ethnic minority migrants,minority workers from rural areas,and ethnic minorities to seek medical treatment and care.
2.2.Instruments
The Chinese version of the Transcultural Self-Efficacy Tool(TSET)scale was translated from the English version of the TSET prepared by Jeffreys [16].The TSET is mainly used to measure and evaluate health service providers’ self-confidence in using transcultural nursing skillsto treat patients with cultural differences.Many scholars have used the TSET to measure the transcultural self-efficacy perceptions of nursing students and nurses [16,21].
In this study,we obtained a research license from Springer publishing company.Following the Brislin [22]two-person translation and retranslation model,consult an expert to ensure cultural accommodation of the scale.In the first step,TSET was translated into Chinese by the researcher and an English major teacher respectively,and the two of them discussed,evaluated and revised together.Secondly,an American English teacher who was familiar with Chinese and a nursing researcher who was proficient in English work together and independently translated the Chinese version of TSET into English on the basis that they had not seen the English version of TSET.In the third step,the translator and the team members compared the accuracy of the two translated versions,and compared the translated versions with the items of the original English scale,looking for differences.The fourth step is to evaluate the translation quality and content validity of the final Chinese version of TSET by an expert committee composed of translators,study group members and specially invited nursing as well as psychology experts.Finally,20 nurses were organized to discuss the expressions of the items in the scale,so that the expressions were closer to Chinese expression habits and easier to understand.
The final TSET-CV contains two parts.The first part is a demographic questionnaire,which collects information about participants’ age,gender,citizenship,marital status,educational background,employment type,working department,working experience,professional title,job title,and monthly income.The second part includes three subscales and 83 items in total.Likert scales ranging from one to ten were used in this study(1=no selfconfidence,10=very confident).The cognitive subscale(25 items)measures how cultural knowledge confidence may influence nursing care for clients of different cultural backgrounds.The practical subscale (30 items)measures confidence in interviewing clients of different cultural backgrounds to learn their values and beliefs.The affective subscale (28 items)measures degree of confidence in identifying values,attitudes,and beliefs concerning cultural awareness,acceptance,appreciation,recognition,and advocacy.The SEL was calculated as follows:a)low (nurses who selected a 1 or 2 response on 80%or more of the subscale items);b)high(nurses who selected a 9 or 10 response on 80%or more of the subscale items);and c)moderate(nurses who selected a 3 through 8 response on 80%or more of the subscale items or who did not fall into the low or high group).The SEST scores were calculated by totaling the subscale item responses and dividing the result by the number of subscale items,resulting in the mean score [16].
The original authors of the scale and subsequent researchers have confirmed that the TSET has good reliability and validity[16,23-25].A factor analysis conducted by Jeffreys and Dogan[25]showed that the overall reliability of the TSET was 0.99.The reliabilities of the three components ranged between 0.95 and 0.99.Halter reported that the overall reliability of the TSET was 0.95[23].In this study,the reliability the TSET-CV scale was consistent with the previous findings.The overall Cronbach’s alpha was 0.987.The coefficient alphas of the cognitive subscale,the practical subscale,and the affective subscale were 0.968,0.979,and 0.968,respectively.
2.3.Data collection
All of the investigators received standardized training before the survey was conducted.Subsequently,the nurses were asked to independently and anonymously complete the questionnaires.The collected questionnaires were screened to exclude those with incomplete responses to the demographic items.All of the instruments could be completed within 30-40 min.The process of the questionnaire collection lasted for two months.A total of 1,265 questionnaires were recovered.Among the 1,265 questionnaires,1190 questionnaires were valid,yielding a recovery efficiency of 96.5%.Nurses voluntarily participated in this survey.
2.4.Data analysis
In this study,SPSS 22.0 software was used for statistical analysis.SEL analysis was frequency statistics-based.T-tests and F-tests were used for the SEST analysis.The aims of these tests were to examine whether there were significant differences in the means among the tested groups according to demographic variables.P<0.05 and P<0.01 were considered statistically significant.
3.Results
3.1.Sample characteristics
Table 1 showed one thousand and ninety nurses completed valid questionnaires.Their average age was 29 (SD=6.79)years.Participants included 1,157 females (97.2%)and 33 males (2.8%).One thousand and six nurses (92.9%)had received a bachelor’s degree or above,and 84 nurses (7.1%)had received secondary vocational education.Among the participants in this study,32(2.7%)were head nurses.Five hundred and sixty-two nurses(47.2%)had no professional title;489 nurses (41.1%)had junior titles;and 139 nurses(11.7%)had intermediate and senior titles.Four hundred and thirty-five nurses (36.6%)worked in departments of internal medicine;500 nurses (42%)worked in surgery departments;121 nurses (10.2%)worked in emergency rooms;33 nurses (2.8%)worked in pediatrics departments;and 101 nurses(8.5%)worked in intensive care units.One hundred and sixteen nurses (9.7%)received an income of less than $400 per month;906 nurses(76.4%)received $400-$1000 monthly;and 168 nurses (14.1%)received more than$1000 monthly.Nine hundred and thirty-three nurses (78.4%)were Han Chinese;257 nurses (21.6%)were of an ethnic minority background.Five hundred and thirty-two nurses(44.7%)were single;636 nurses (53.4%)were married;and 22 nurses (1.8%)were divorced.Two hundred and fifty-two nurses(21.2%)were hospital employees;and 938 nurses (78.8%)were temporary nurses.
3.2.The constituent ratio of transcultural SEL
Based on Jeffrey’s SEL procedure [16],we calculated the distribution of the SEL according to the different subscales.Table 2 showsthe transcultural SEL for the cognitive,practical,and affective subscales among the nurses working in tertiary general hospitals in Guizhou Province,China.The data showed that nurses with moderate SEL were dominant in the cognitive(88.7%),practical(90.8%),and affective subscales (91.6%),respectively.An average of 10% of the nurses had high SEL(cognitive:11.1%;practical:8.9%;affective:8.2%).Nurses with low SEL were rare.Less than 1% of nurses had low SEL on average(cognitive:0.3%;practical:0.3%;affective:0.2%).
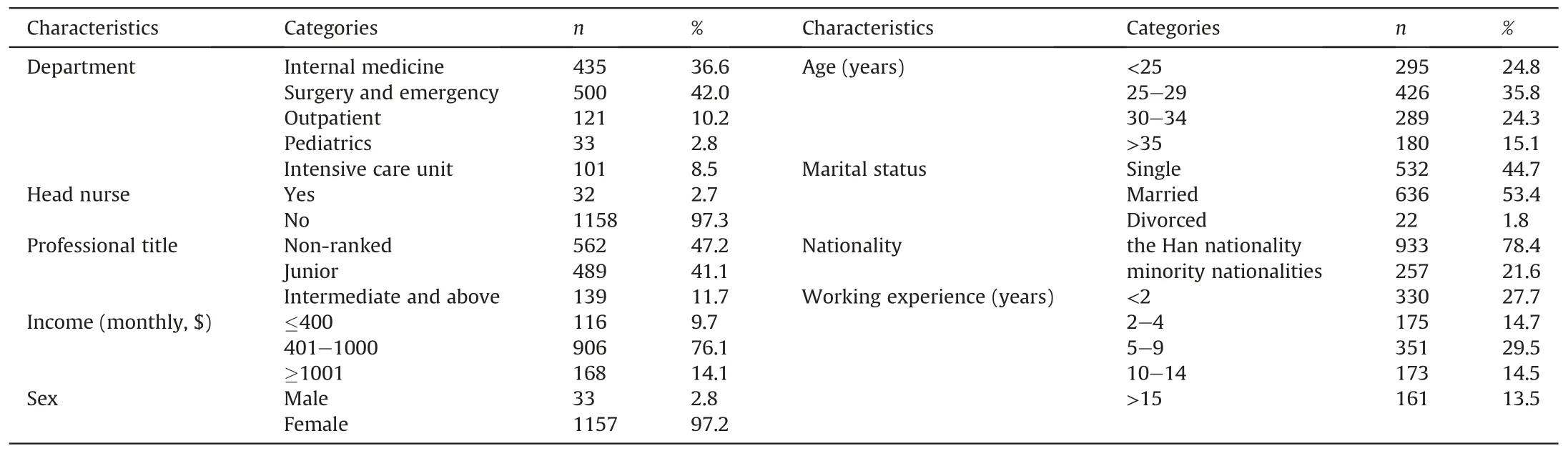
Table 1 Sample characteristics.
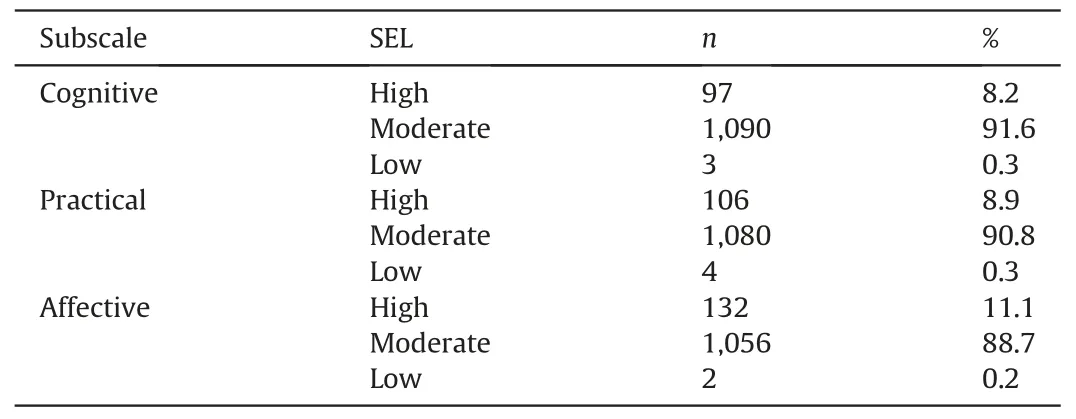
Table 2 Perceived self-efficacy level distributions (N=1190).
3.3.Transcultural SEST and its influencing factors
No significant difference in SEST scores was found between the genders or among the educational backgrounds for the three subscales.However,age,marital status,employment type,professional title,monthly income,department,and whether they were head nurses resulted in significant differences in SEST scores.
Based on the demographic data table in Jeffreys’s study[21],we divided the nurses into four age groups.Table 3 shows the SEST scores of the nurses according to the age group for each of the three subscales.Significant differences in SEST scores were found among the age groups for both the cognitive and affective subscales but not for the practical subscale.A post-hoc test showed that nurses under 25 years old had lower SEST scores on the cognitive subscale than any other age groups.On the affective subscale,nurses older than 35 years had significantly higher SEST scores than the other age groups.
Table 3 shows the SEST scores of nurses by marital status for the three subscales.Significant differences in SEST scores according to marital status were found for the cognitive and affective subscalesbut not for the practical subscale.The results of a post-hoc test showed that the SEST scores of married nurses were significantly higher than those of single or divorced nurses for the cognitive subscale.In addition,the SEST scores of married nurses were significantly higher than those of single nurses on the affective subscale.
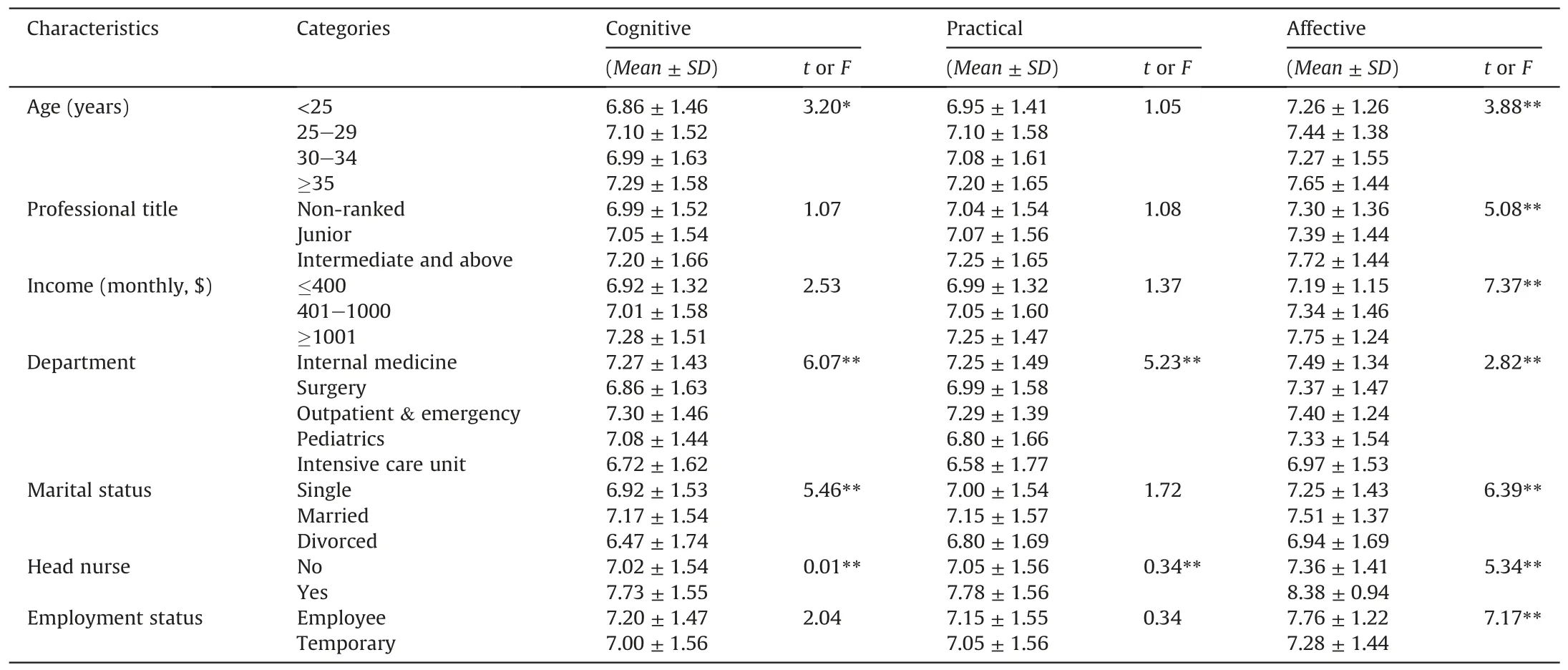
Table 3 Participant characteristics and Transcultural Self-Efficacy Test (TSET)scores.
Table 3 shows the SEST scores by employment type for each of the three subscales.Temporary workers and formal employees most significantly different on the affective subscale;the SEST scores of the hospital employee nurses were higher than those of the temporary nurses.No significant difference in SEST scores was found between the two types of employment for either the cognitive or practical subscales.
Table 3 also shows the SEST scores by professional title for each ofthe three subscales.Nurses with non-ranked titles had the lowest SEST scores on all of the subscales.On the affective subscale,significant differencesin SEST scores was found among the professional titles.The results of a post-hoc test showed that nurse practitioners and above had significantly higher SEST scores than nurses with the other two professional titles.For the cognitive and practical subscales,no significant differences in SEST scores were found to be associated with nurses’ professional titles.
With regard to monthly income,significant difference sin SEST scores on the affective subscale were found among nurses with different monthly incomes.However,on the cognitive and practical subscales,no significant difference in SEST scores was found.A post-hoc test showed that the nurses with the highest monthly income (more than $1,000)had significantly higher SEST scores than the nurses in the other two income groups.
The SEST scores of nurses working in different departments differed significantly for each of the three subscales.A post-hoc test showed that nurses working in the outpatient emergency rooms had the highest SEST scores on the cognitive and practical subscales,while nurses working in the intensive care units had the lowest SEST scores.Nurses working in the departments of internal medicine had the highest SEST scores on the affective subscale,while nurses working in the intensive care units had the lowest SEST scores.As shown in Table 3,the SEST scores of head nurses and other nurses significantly differed on all three subscales;the SEST scores of the head nurses were significantly higher than those of other nurses.
4.Discussion
This study demonstrated that the transcultural SEL of the nurses was generally moderate.And the results were roughly the same as those reported by Ju-hyun Jin[26],He reported the majority of the staff nurses belong to the medium level group of TSE in the SPC Health Care-Ministry Hospitals.According to Leninger [9]and Cronin and Harrison [2],differences among ethnic minority cultures,subcultures,and mainstream cultures of patients from diverse communities within a countryshould also be included in studies of transcultural nursing.Berry and Sabatier [27]also consider that,similar to international migrants,there are also cultural differences among migrants within a country.Therefore,this study used nurses as research subjects to study the transcultura lself-efficacy of nurses who received nursing training based on a mainstream cultural perspective and who provided healthcare to resident ethnic minorities.
According to the hypotheses of previous studies [23,25,28],there is an important relationship between SEL and experience.The presence of inordinately high or low SEL in nursing students was primarily caused by overconfidence or lack of confidence due to lesser or total lack of work experience.In China,the number of patient population is enormous.Each hospital examined in this study serves approximately 10,000 outpatients and 3,000 hospitalized patients per day.Nurses regularly encounter the cultural differences of patients of different ethnicities,languages,religious beliefs,and values.These conditions allow nurses to accumulate abundant work experience.Therefore,it is reasonable that only a few nurses showed low transcultural SEL and that most of the nurses showed moderate transcultural SEL in this study.The results indicate that clinical nurses working in high-volume hospitals are more likely to objectively and rationally assess their own performance.However,this finding also revealed another issue:few nurses had high transcultural SEL,suggesting that the nurses still had insufficient self-confidence to address patients with different cultural backgrounds.This result is similar to Joanne’s study [29],He thought that transcultural self-efficacy may be influenced by formal education and learning experiences of DNP students.It is possible that this lack of confidence was associated with the nursing education system in China.Although transcultural nursing has been practiced in China for a long time,nursing education places too much focus on basic medicine with no specific curriculum that focus on culturally competency training.Transcultural nursing content is rarely featured in continuing education programs in hospitals,which results in inadequate multicultural nursing content in nursing education in China.Chinese nursing educators are aware of these issues and are making effort in improving this aspect of nursing education.
In this study,the second research objective was to investigate the effect of demographic variables on nurses’ transcultural SEST.No significant difference in SEST scores was found between genders or among nurses with different educational backgrounds on any of the three subscales.However,significant differences in SEST scores were found based on age,marital status,employment type,professional title,monthly income,working department,and job duties.We have reported the results of measuring the crosscultural self-efficacy of nurses in Guangzhou,China [30].Older nurses—those with more years of work experience,higher professional titles,and higher incomes—and those from a minority background and who are officially employed have high perceived transcultural self-efficacy.We found that in addition to marital status,the self-efficacy of nurses measured in the two provinces was relatively similar to other demographic categories,so the cross-cultural self-efficacy of nurses in different regions of China should be at a relatively stable level.
This study found that nurses younger than 25 had the lowest self-efficacy scoreson each of the three subscales,while nurses older than 35 had the highest scores.Presumably nurses with a longer working history are more likely to have cumulative nursing experiences in clinical practice.The data appeared to indicate that transcultural self-efficacy increases with age.This result reinforces the message that nursing experience is important to the nurses’transcultural self-efficacy.
The results also showed that married nurses had significantly higher SEST scores than single or divorced nurses.Married nurses were relatively older than single nurses and had worked more years and had a more abundant nursing experience,which explains their higher SEST scores.These results are consistent with the important association between experience and SEST proposed by Jeffreys et al.These findings also suggested that stable marital status is favorable to higher SEST scores among nurses.
Moreover,this study demonstrated that the higher the nurses’monthly income,the higher the SEST scores.A significant difference in the SEST scores on the affective subscale was also found among nurses with different monthly incomes.Nurses who were hospital employees had higher SEST scores than temporary nurses on each of the three subscales.Significant differences in SEST scores for the affective subscales were also found between these two types of employment.
Regarding professional titles,non-ranked nurses had the lowest SEST scores while nurses who were nurse practitioners or above ranks had the highest SEST scores.In China,a professional title reflects nursing competence.It is also an integrated representation of professional knowledge,technical merit,and research capacity[31].
This integrated representation is worth further discussion.Although we could speculate that higher incomes lead to higher SEST scores,an in-depth data analysis showed that 86 nurses with the highest monthly incomes had three characteristics.First,this group of nurses had received bachelor’s degree or higher.Among this group of nurses,51.2% were hospital employees and had intermediate or higher professional titles.Their educational backgrounds,professional titles,and employment types were therefore better than those of other groups.These characteristics coincided with the human resource management system used among nurses in China,in which a nurse’s income,employment type,and professional title are closely related.The overall educational backgrounds of employee nurses are higher than that of temporary nurses.Moreover,formally employed nurses have priority access to the continuing education,professional development,job promotion,and other opportunities offered by their hospitals.They experience no risk of being laid off,therefore,have a relatively stable work environment.Second,81.4%of the nurses in this group were 35 years or older,indicating that they belonged to the most experienced and energetic age group of Chinese nurses.Third,the vast majority of the nurses(91%)were married.Married individuals may have a higher level of social support and thus result in better emotional status.According to Bandura’s self-efficacy theory [10],emotional status plays an important role in self-efficacy.When an individual encounters stress or a threatening environment or emotion,his or her inefficacy will lead to anxiety,fear,depression,and other negative emotions.These issues further weaken the enthusiasm of individual behaviors and hinder the normal performance of various psychological functions.In contrast,high efficacy leads to positive emotional experiences,such as self-confidence.Therefore,it is possible thata stable work environment,being married,a higher level of education,and relatively high professional title are favorable to the cultural self-efficacy of nurses.The direct correlation between higher income and higher efficacy was only a superficial phenomenon caused by the combined effect of the above factors.
Another interesting finding of this study was that nurses working in different departments,including internal medicine,surgery,outpatient emergency room,pediatrics,and intensive care,had significantly different SEST scores on each of the three subscales.Nurses working in the intensive care unit had the lowest SEST scores on each subscale,followed by nurses working in the pediatrics departments.Because patients in the intensive care units are typically in critical condition or in a coma,nurses may have difficulty communicating with them and instead rely on the functional nursing model.Due to a long-term lack of effective communication with patients and the challenges of transcultural nursing,nurses working in intensive care units were found to lack cognitive competence in cultural nursing.Nurses in the pediatric departments usually treat juvenile patients and have relatively fewer opportunities to communicate with them.Hence,the cultural sensitivity and awareness of nurses in the pediatrics department is relatively low.In contrast,nurses working in the internal medicine,surgery,and outpatient emergency departments are more likely to communicate and interact with patients with cultural differences.Therefore,their SEST scores were relatively higher than those of the nurses working in the intensive care units and pediatric departments.The SEST scores of nurses working in the outpatient emergency rooms were significantly higher than those of nurses working in other departments.Because emergency rooms are where outpatients are admitted to the hospital,numerous patients with cultural differences visit and are diverted from the emergency room to different departments every day.Therefore,these nurses reported a greater capacity to respond to patients with cultural differences.The data from this study showed that the SEST scores of nurses working in inpatient clinical departments were lower than those of nurses working in the outpatient emergency room.Because Bandura’s[10]theory suggests that direct behavioral experience is an important factor in enhancing self-efficacy and the most influential factor in the formation of self-efficacy,we speculate that nurses working in the outpatient emergency rooms encounter more patients with cultural differences and therefore accumulate cultural nursing experiences during their daily tasks.
This survey also showed that the SEST scores of the head nurses were significantly higher than those of the other nurses on each of the three subscales.Head nurses are managers and have relatively stronger motivation and awareness,which helps them learn more quickly.They are also generally more comprehensively skilled than other nurses and have more confidence in their professional competence.Based on Bandura’s self-efficacy theory,we concluded that the higher a nurse’s ability,the stronger the nurse’s confidence in being able to achieve specific goals.
Unlike nursing students in schools,nurses have only one option for improving their clinical transcultural ability and perceived transcultural self-efficacy,namely,through in-service continuing education.Nurses in Chinese hospitals have no opportunity for transcultural education when they are students,and therefore,their overall transcultural SEL is not high.The results also inspired suggestions for China’s nursing education programs:transcultural nursing courses should be included in nursing education programs.These courses should be taught one year before graduation to help student nurses better learn and master transcultural nursing skills during practical training and thus have a higher level of transcultural nursing self-efficacy and capability when they become nurses.Hospital nursing management should offer continuing education on transcultural nursing appropriate to the demographic characteristics of the nurses to make up for the missed education to some extent,so that nurses can provide high-quality transcultural nursing to patients for decades of working life to come.
In this study,the reliability the TSET-CV scale was consistent with the previous findings.The overall Cronbach’s alpha was 0.987.The coefficient alphas of the cognitive subscale,the practical subscale,and the affective subscale were 0.968,0.979,and 0.968,respectively.Compared to a study by an author in Shanghai,China,the study reports thehe overall Cronbach’s alpha was 0.99.The coefficient alphas of the cognitive subscale,the practical subscale,and the affective subscale were 0.91,0.91,and 0.92,respectively.The similarity between the two studies indicates that the scale is relatively close and stable in measuring the cross-cultural self-efficacy of Chinese nurses.
5.Conclusions
This study demonstrated that the transcultural SEL of the nurses was generally moderate;few nurses had a high or low transcultural SEL.The SEST scores of the nurses were affected by age,marital status,employment type,professional title,income,work experience in different departments,and job title.Nursing management in hospitals should offer continuing education on transcultural nursing according to nurses’ demographic characteristics and the SEST scores.Nursing administrators in hospitals can combine the characteristics of transcultural self-efficacy among different groups of nurses to explore the establishment of methods for improving cultural competency.Transcultural skills and knowledge can also be integrated into the continuing education system for hospital nursing.Relevant evaluation systems can also be gradually introduced into nursing management practices.Doing so will compensate for the transcultural nursing education that nurses miss as students and will improve nurses’ perceived transcultural selfefficacy and transcultural nursing capability to enable them to provide quality nursing to the increasing number of patients from different cultures.
CRediT authorship contribution statement
Juan Li:Writing -original draft,Conceptualization,Methodology,Software.Bei Wu:Writing -review &editing,Conceptualization,Methodology.Zhuang He:Software,Supervision.Jiru Liu:Software.Rong Xiao:Visualization,Investigation.Yong Luo:Visualization,Supervision.
Acknowledgement
We express deep gratitude to Professor Marianne Jeffreys and to Springer Publishing Company for providing the TSET tool and technical support.This study has no conflicts of interest with other papers,studies,authors,and publishers.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.03.004.
 International Journal of Nursing Sciences2020年2期
International Journal of Nursing Sciences2020年2期
- International Journal of Nursing Sciences的其它文章
- Exercise for fatigue in breast cancer patients:An umbrella review of systematic reviews
- Antiretroviral therapy improves neurocognitive impairment in people living with HIV? A meta-analysis
- Intervention effect of neuromuscular electrical stimulation on ICU acquired weakness:A meta-analysis
- Psychometric properties of the Chinese Version of the Readiness for Hospital Discharge Scale for people living with HIV
- Experiences of graduates in Massachusetts of the United States from a RN-to-BSN program
- Analysis on nursing competence and training needs of dementia caregivers in long-term care institutions