
Applications of mPCR testing reduced initial antibiotic use and duration of mechanical ventilation in virus-infected children with severe community-acquired pneumonia admitted to the PICU
2022-06-27 11:10:38NanFanBoLiangFCahnagoHengMiaoGaoRuBoLiGuoYunSuYiYangMaoYuShanHeYueWangXiaoHeZhouLiangMingCaiYeQingwangJenniferBlumenthalSuYunQian
World Journal of Pediatrics 2022年6期
-Nan Fan ·Bo-Liang FCahnago.Heng-Miao Gao.Ru-Bo Li. Guo-Yun Su.Yi-Yang Mao.Yu-Shan He.Yue Wang.Xiao-He Zhou.Liang-Ming Cai.Ye-Qing wang.Jennifer A. Blumenthal.Su-Yun Qian
Community-acquired pneumonia (CAP) remains the leading cause of morbidity and mortality among children worldwide. It is critical for these patients to select and timely initiate appropriate empirical antimicrobial therapy against the causative pathogens [ 1]. However, conventional pathogendetecting methods, such as culture and serology, have no prospect of altering empiric therapy owing to their time delay in obtaining results and to their lower detection rates [ 2]. Recent advances in molecular diagnostic assays, such as multiplex polymerase chain reaction PCR (mPCR) methods, have been used to detect multiple pathogens in CAP simultaneously within two hours and have dramatically improved the ability to diagnose respiratory pathogens [ 3]. However, whether this molecular diagnosis method can reduce the use of antibiotics and can improve prognosis in severe CAP children, especially those less than 5 years old, remains to be explored.
We conducted a retrospective cohort study enrolling 219 children with severe CAP in the pediatric intensive Care Unit (PICU) between 1 January 2016 and 31 December 2018, including 151 patients in the traditional testing group and 68 in the mPCR testing group. Respiratory samples from all patients were collected within 12 hours of admission to PICU. In the traditional testing group, routine microbiological methods were performed and children received empirical antimicrobial treatment. In the mPCR testing group, children underwent the mPCR testing within 12 hours of admission to PICU and selective use of antibiotics according to the rapid pathogen detection results.
About 77% (169/219) of patients were under 5 years; and there was no significant difference in the median age of these two groups. The gender composition was also similar. Other baseline clinical characteristics and laboratory results did not differ significantly between these two groups (Table 1).
The etiological identification rate in the traditional and mPCR testing groups were 72.4% and 77.8%, respectively, of which bacterial infections (42.9% vs. 47.1%), viral pathogens (51.0% vs. 55.9%) andmycoplasma pneumonia(15% vs. 17%) were determined. No significant differences were detected in the distribution of viral and bacterial pathogens between these two groups. In both the traditional and the mPCR testing groups, the most common bacteria found wereS. pneumoniae(20% vs. 19%),S. aureus(14% vs. 21%), andH. influenza(18% vs. 13%). The most common viruses were respiratory syncytial virus (43% vs. 45%) and influenza (42% vs. 30%), respectively (Table 2). The detection rate of coronavirus was only 8% in the mPCR testing group, and coronavirus was not tested for the traditional testing methods.
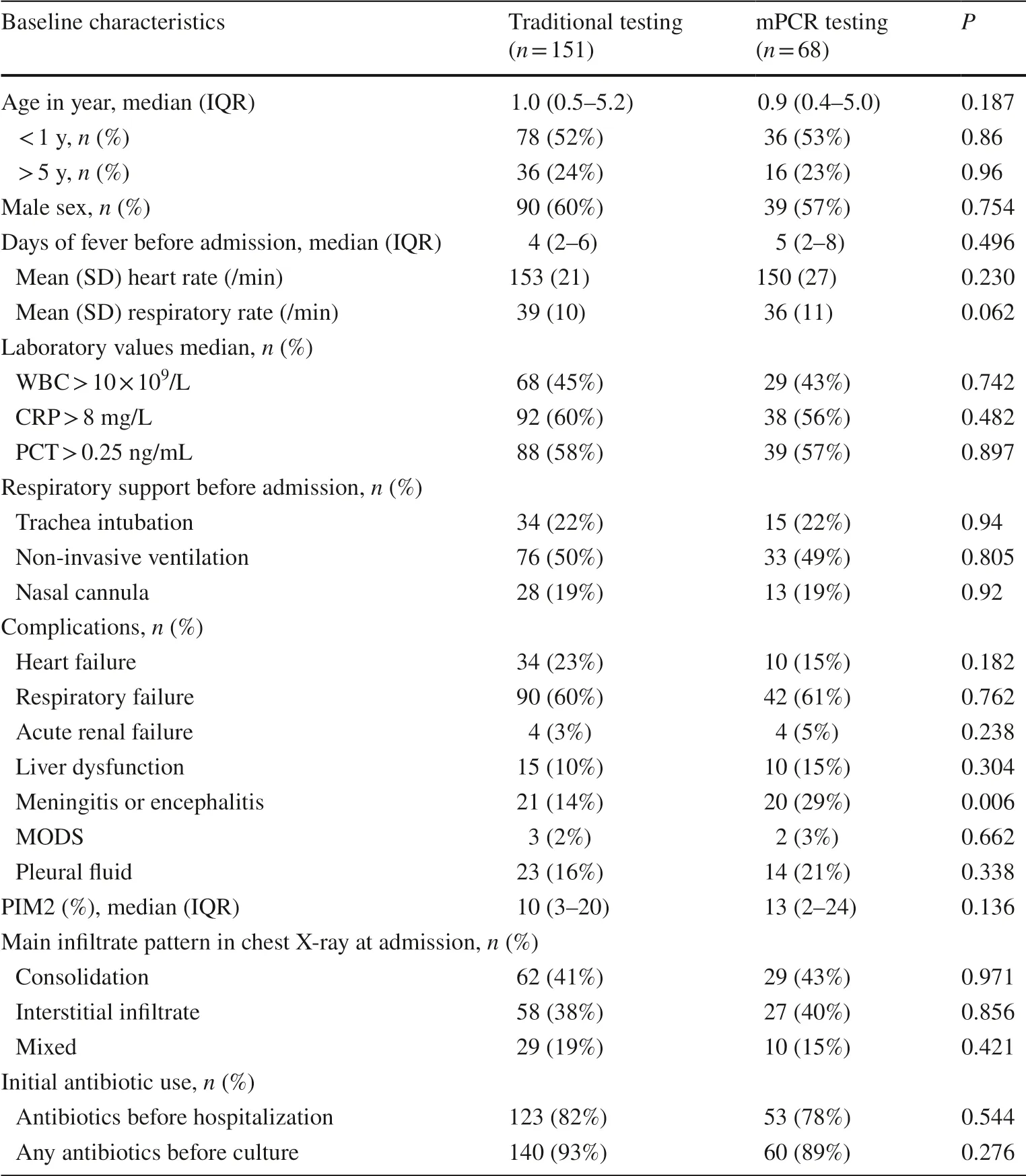
Table 1 Patient demographics and clinical characteristics
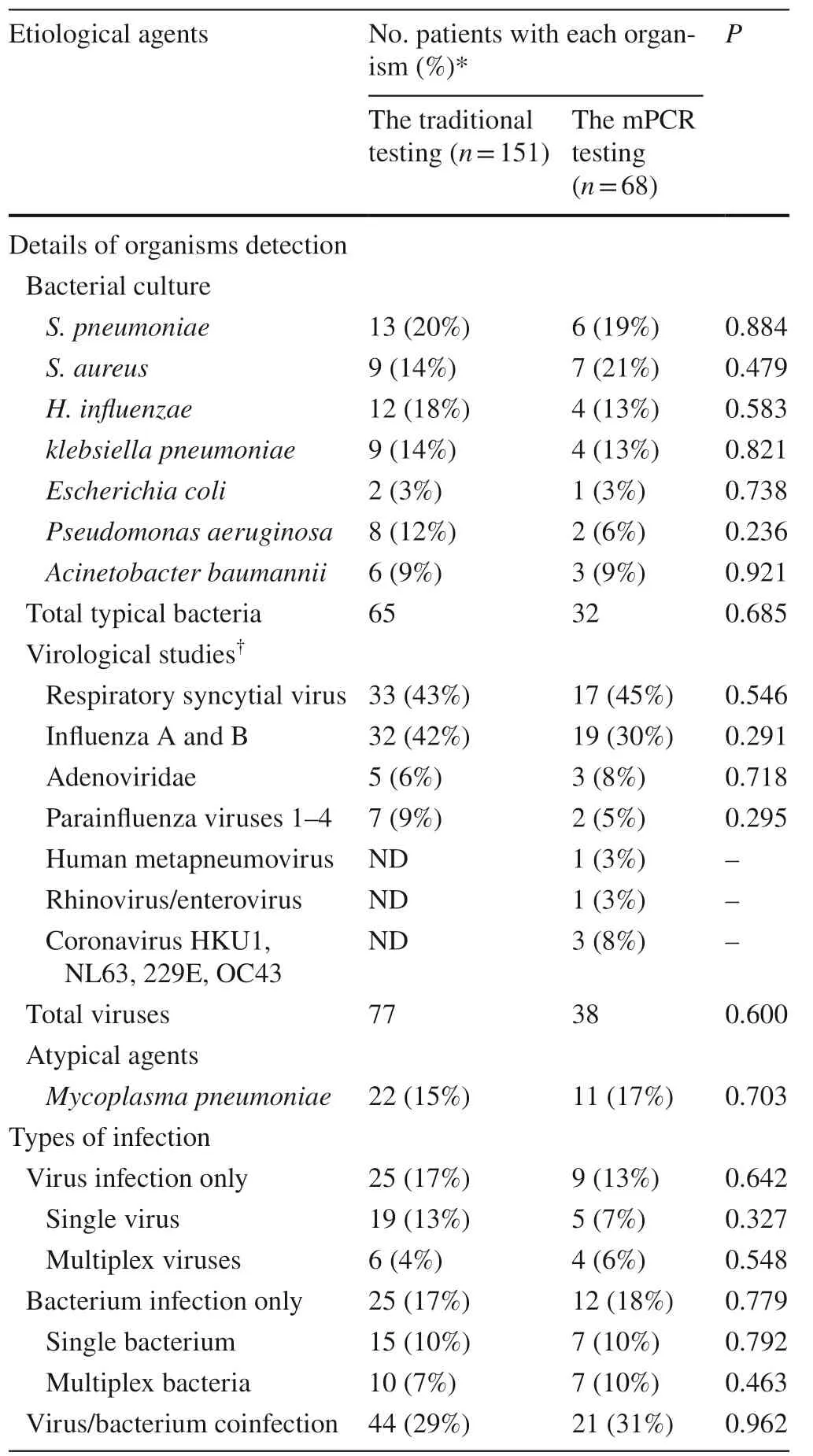
Table 2 Microbiological yield in the study population
Initial antibiotic therapy at PICU admission was 56.6% (124/219), of which 86/151 (57.0%) was determined by traditional testing method and 38/68 (55.9%) by mPCR testing method. In patients with mPCR diagnosed with viral infection, initial antibiotic use (38%) was lower than that of the traditional testing group (78%) (P= 0.023). This was especially true of cephalosporin use, which reduced from 33% (traditional group) to 6% (mPCR group) (P= 0.043). Use of one antibiotic reduced from 37 to 19%, and use of two antibiotics reduced from 33 to 13%, but without statistical significance between the traditional and mPCR testing groups. Antibiotic treatment was similar between the two groups with bacterial infection and viral/bacterial coinfection.
No significant differences were observed in the percent of invasive mechanical ventilation used, length of hospital stay, and PICU stay between the traditional and mPCR testing groups. However, in patients with only viral infection or viral/bacterial coinfection, duration of mechanical ventilation was 5 days (range 3–7 days) and 12 days (range 4–16 days) in the traditional testing group, and it decreased to 3 days (range 1–5) and 7 days (range 3–9) in the mPCR testing group.
Although several observational studies have shown that mPCR detection of respiratory viruses has an impact on reducing the use of antibiotics in patients with viral pneumonia, there are fewer reports on children under 5 years of age [ 4– 6 ]. In our study, most children were under 5 years of age and were discharged with a primary diagnosis of severe CAP. Similarly, the mPCR testing method has slightly increased the capability of identifying pathogens and has reduced initial antibiotic prescribed among children with viral infection [ 5, 6]. Pathogen-directed therapy can avoid unnecessary antibiotic or antiviral use, can facilitate more timely and effective use of drugs, and can help to prevent the secondary spread of infection, all of which contribute to shorten the length of hospitalization and to significantly influence patient management and disease prognosis [ 7].
Our study revealed that the mPCR testing method was associated with a significantly decreased duration of mechanical ventilation in patients with viral infection or viral/bacterial coinfection. Specifically, patients with bacterial infections tended to have a more severe course according to PICU admission rates, respiratory support necessity, clinical disease severity scales and length of hospitalization [ 8]. Previous research shows that the occurrence of pathogens with high antibiotic resistance in the lower respiratory tract increases with increased duration of hospital care and mechanical ventilation [ 9]. Alternatively, knowledge of a reduced duration of ventilation can be used to justify a prospective trial to assess the proper employment of antibiotics in children with severe CAP requiring invasive ventilation [ 10].
In the future, greater use of PCR amplification of bacteria may be accompanied by precise antibiotic prescription and can provide comprehensive information related to etiology in children with severe CAP.
Acknowledgements The authors of this paper would like to thank all the staff at the Diagnostic Microbiology Laboratory, and appreciate the work of nurses and doctors in Pediatric Intensive Care Unit in Beijing children’s Hospital.
Author contributions SQ participated in the study concept and design, revising this article critically for important intellectual content, and final approval of the version to be published. JB participated in the revision of the paper and final approval of the version to be published.CF carried out study design, the acquisition of date, analysis and interpretation of data, and drafted the manuscript. BF participated in the study concept and design. GS, RL, YM, YH, YW, XZ, LC made substantial contributions to acquisition of data, or analysis and interpretation of the data. HG participated in the critical revision of the manuscript. All authors read and approved the final manuscript.
Funding This study was supported by pediatric special project from pediatric discipline collaborative development center of Beijing hospital management center (XTZD20180504) (S. Q).
Data availability statement The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of interest No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Ethical approval The study protocol was reviewed and approved by the ethics committee of Beijing Children’s Hospital (2018-k-103).
Informed consent Written informed consent was obtained from parents when laboratory testing for research purposes is done.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/.
 World Journal of Pediatrics2022年6期
World Journal of Pediatrics2022年6期
- World Journal of Pediatrics的其它文章
- Instructions for Authors
- Serum homocysteine, lipid profile and BMI as atherosclerotic risk factors in children with numerical chromosomal aberrations
- Neonates are more vulnerable to symptomatic SARS-CoV-2 infection than children: a matched cohort study in Brazil
- Trichotillomania occurs during the COVID-19 pandemic in an adolescent
- Short-term effects of air pollutants on hospital admissions for acute bronchitis in children: a multi-city time-series study in Southwest China
- Impact of rotavirus vaccine implementation on Israeli children: a comparison between pre- and post-vaccination era