
Effect of early atopic sensitization in children aged 0–2 years on the development of asthma symptoms at 9–11 years of age
2022-11-18 02:16:42HimmetHalukAkarEbruNadirBurinBekenYakupYeil
World Journal of Pediatrics 2022年11期
Himmet Haluk Akar ·Ebru Nadir·Bur?in Beken ·Yakup Ye?il
Abstract Background Personal genetic predisposition and early life environmental factors are important for the development of childhood asthma.We aimed to search whether egg,milk and mite sensitizations at 0–2 years old are risk factors for asthma symptoms at 9–11 years old.Methods A total of 210 wheezer children who had specific immunoglobulin (Ig) E in 2010–2012 were included in the study(followed by pediatric allergy).Patients were divided into non-atopic (group 1,n =157) and atopic patients [groups 2–7,n =53 (5 patients were in both group 4 and group 5)] based on sensitizations.Using the International Study of Asthma and Allergy in Childhood questionnaire,current wheeze (CW,2nd question),exercise wheezing (EW,7th question),and dry cough (DC,8th question) were surveyed.Also,parental allergies,eczema at 0–2 years,current eosinophil percentage and total IgE were recorded.Results Eczema was observed as an important risk factor [CW: odds ratio (OR)=2.83,95% confidence interval (CI)=1.54–5.23,P ≤ 0.001;EW: OR=2.71,95% CI=1.33–5.54,P =0.006;DC: OR=3.03,95% CI=1.47–6.25,P =0.003],whereas having no atopic sensitization at 0–2-year-old (group 1) was found as a significant protective factor for asthma at 9–11 years old (CW: OR=0.32,95% CI=0.15–0.70,P =0.004;EW: OR=0.21,95% CI 0.10–0.44,P ≤ 0.001;DC:OR=0.25,95% CI=0.10–0.59,P =0.002).Conclusion Early personal eczema is a significant risk factor for the development of asthma symptoms at 9–11 years old,whereas not having an allergic sensitization at 0–2 years old (group 1) is an important protective factor.
Keywords Asthma·Children·Risk factors
Introduction
During the last three decades,the increasing prevalence of childhood asthma is a known fact throughout the world,especially in developed countries [1].The interaction between genetic predisposition and early life environmental factors is thought to be associated with the development of later life childhood asthma symptoms.However,information on the occurrence of these interactions still remains unclear.In children,while some environmental factors such as early atopic sensitization,viral respiratory infections,passive tobacco smoke exposure,and pet contact can be predisposing risk factors,large family size,rural life,and animal contact can be protective factors for the development of subsequent asthma symptoms [2].The association between early life atopic sensitization and the development of later life asthma have frequently been investigated in birth cohort studies [3–5].Data from the Isle of Wight(IoW) birth cohort (1456 infants) showed a strong association between atopic sensitization (common food-allergens or aero-allergens) at 4 years old and asthma at 10 years old[3].The German Multicenter Allergy study (1314 infants)in fact showed that only persistently sensitized children(i.e.,children who were sensitized to any allergen early in life and who were sensitized to inhalant allergens by the age of 7 years) were at a significantly increased risk of being asthmatic at the age of 7 years [odds ratio (OR)=10.12,95% confidence interval (CI)=3.81–26.88,compared with never being sensitized children].Furthermore,food sensitization in the first two years of life (without aero-allergen sensitization: OR=2.21,95% CI=0.78–6.29;with aeroallergen sensitization: OR=11.10,95% CI=4.73–26.07)was a strong predictor for development of asthma,but inhalant sensitization without concurrent food sensitization in the first two years of life was not (OR=0.85,95%CI=0.11–6.51) [4].In another study,Simpson et al.[5],used machine learning methods to cluster children from the Manchester Asthma and Allergy study birth cohort (1186 infants) into five atopic clusters and found that the children with multiple early sensitizations were most likely to have persistent wheezing at 8 years old.Also,sensitization to food-and aero-allergens were included to the modified Asthma Predictive Index (mAPI) as a minor and as a major factor,respectively [6].
The aim of the present study was to investigate the association between the early allergen sensitization at the 0–2 years of age and the development of asthma symptoms at 9–11 years of age.We hypothesized that there is a high prevalence of asthma symptoms at 9–11 years old in children having egg,milk and mite sensitization at 0–2 years of age.
Methods
The study was conducted in Istanbul Health Sciences University,Kanuni Sultan Suleyman Training and Research Hospital between June 2021 and November 2021 (approval number: KAEK/2022.01.5).The medical records of a total 210 wheezers aged 0–2 years who attended the paediatric allergy clinic between 2010 and 2012 were analyzed to assess the relationship between early life sensitization and asthma symptoms at 9–11 years old.The patients were classified based on their serum specific immunoglobulin E (sIgE) levels[hen’s egg white (F1),cow’s milk (F2),dermatophagoides farinea (D1) and dermatophagoides pteronyssinus (D2)]into non-atopic (group 1) and atopic groups (groups 2–7).The definition of groups is detailed in the relevant section below.After study design,we contacted patients’families via phone and invited them to hospital for evaluation including International Study of Asthma and Allergy in Childhood (ISAAC) questionnaire.A structured form was completed with the patients and/or parents at the interview.This form included current age,gender,type of birth (vaginal or caesarean section),family history of allergy (asthma,allergic rhinitis,eczema in mother or father,or asthma in sibling),eczema at 0–2 years old,current eosinophil percentage,and current total IgE levels.Also,the ISAAC questionnaire was completed for asthma symptoms at 9–11 years old.Based on the ISAAC questionnaire,we abbreviated three questions of the survey as “current wheeze” (CW;wheeze in the prior 12 months,2nd question),“exercise wheezing” (EW;wheeze during or after exercise in the prior 12 months,7th question) and “dry cough" (DC;dry cough at night in the prior 12 months,8th question) (Supplementary Table 1) [7].
The sIgE levels were measured by Immuno-CAP assay(Phadia US Inc,Portage,MI).The Immuno-CAP testing results were accepted as positive for values ≥ 0.35 kU/L.F1,F2,D1,D2 and F5 [food panel that include F1,F2,F4(wheat),F13 (peanut),F14 (soybean)] tests were investigated using atopic sensitization screening in the Istanbul Health Sciences University,Kanuni Sultan Suleyman Training and Research Hospital.The level of total IgE was detected with nephelometric method.The percentage of eosinophil was obtained from the complete blood count.
Definitions
(1) Eczema: chronic relapsing itchy dermatitis (lasting > 6 weeks) with characteristic distribution;(2) maternal/paternal allergy and/or sibling asthma: the presence of doctor diagnosed allergic diseases (asthma,and/or allergic rhinitis,and/or eczema) in mother and father and doctor diagnosed asthma in siblings;(3) group 1 (non-atopic/nonsensitizer): the level of sIgE < 0.35 kU/L for any of F1,F2,D1,D2;(4) group 2 (milk,milk sensitizer alone): the level F2 ≥ 0.35 kU/L without any of F1,D1,D2;(5) group 3 (egg,egg sensitizer alone): the level of F1 ≥ 0.35 kU/L without any of F2,D1,D2;(6) group 4 (milk+egg,milk plus milk sensitizer): level of both F1 and F2 ≥ 0.35 kU/L without D1 and/or D2;(7) group 5 (food allergy): the level of F1 > 2 kU/L and F2 > 5 kU/L at 0–2 years old for egg and milk allergy,respectively [8];(8) group 6 (mite sensitizer alone): the level of D1 and/or D2 ≥ 0.35 kU/L without F1 and/or F2;(9) group 7 (food+mite,food plus mite sensitizer): the level of F1 and/or F2 ≥ 0.35 kU/L plus D1 and/or D2 ≥ 0.35 kU/L;(10) eosinophilia: the percent of eosinophil ≥ 4% in white blood cells at 9–11 years old;(11)elevated total IgE: total IgE levels > 200 IU/L at 9–11 years old.
Statistical analysis
SPSS version 24.0.(SPSS Inc,Chicago,IL) was used for statistical analysis.Two-step statistical analysis was performed in the study.In the first step,univariable analysis was performed with 15 different variables separately in comparison with children who do not have same risk factors.For this purpose,Chi-square test (χ2) was used.In the second step,the binary logistic regression was used to obtain independent effects of these variables.For this purpose,we selected factors with aPvalue ≤ 0.003[(0.05/15=0033,Bonferroni correction),to avoid high type 1 error which was 0.536=1-(1–0.05) 15] from the results of univariable analysis.Also,ORs were used to measure the magnitude of effect for each risk factor.Significant associations were defined withPvalue ≤ 0.05 in all tests.
Results
Two hundred and ten children (125 male,85 female)were included in the study.The mean age of patients was 9.730 ± 0.756 years.The asthma symptoms of CW,EW and DC were present in 45.2% (95/210),29.5% (62/210)and 26.2% (55/210) of all participants,respectively.The same symptoms (CW,EW and DC) and clinical characteristics of patients were shown for all groups in the Table 1.
Risk factors for the development of current wheeze at 9–11 years of age
Risk factors in the univariable risk analysis for CW at 9–11 years old are listed in the Table 2.Having maternal allergy (OR=1.73,95% CI=0.97–3.06;P=0.040),paternal allergy (OR=2.14,95% CI=0.98–4.68;P=0.040),eczema at 0–2 years old (OR=3.58,95% CI=2.00–6.42;P≤ 0.001),group 4 (OR=7.39,95% CI=1.59–34.26;P=0.003),group 5 (OR=6.64,95% CI=1.41–31.13;P=0.006),group 7 (OR=5.19,95% CI=1.07–25.08;P=0.025),eosinophilia (≥ 4%;OR=2.01,95% CI=1.11–3.63;P=0.014) and elevated total IgE (> 200 IU/mL;OR=2.18,95% CI=1.23–3.88;P=0.006) were all found to be significant risk factors for CW.Male gender(P=0.081),caesarean section (P=0.468),having sibling asthma (P=0.343),group 2 (P=0.256),group 3 (P=0.530)and group 6 (P=0.164) did not show any associations with CW.In addition,not having an allergic sensitization at 0–2 years old (group 1: OR=0.22,95% CI=0.11–0.44;P≤ 0.001) was found to be a protective factor for CW in the univariable risk analysis.
Risk factors for the development of exercise wheezing at 9–11 years of age
Risk factors in the univariable risk analysis for EW at 9–11 years old are listed in the Table 3.Having maternal allergy (OR=1.97,95% CI=1.07–3.65;P=0.022),paternal allergy (OR=2.79,95% CI=1.27–6.09;P=0.008),eczema at 0–2 years old (OR=3.16,95% CI=1.70–5.88;P≤ 0.001),group 4 (OR=4.46,95% CI=1.39–14.25;P=0.011),group 5 (OR=3.83,95% CI=1.16–12.59;P=0.026),group 7(OR=6.47,95% CI=1.61–25.94;P=0.007),eosinophilia (≥ 4%;OR=5.52,95% CI=2.81–10.82;P≤ 0.001)and elevated total IgE (OR=1.96,95% CI=1.00–3.83;P=0.032) were found to be risk factors for EW.Male gender (P=0.290),caesarean section (P=0.527),having sibling asthma (P=0.432),group 2 (P=0.057),group 3 (P=0.588)and group 6 (P=0.078) did not show any associations with EW.Not having an allergic sensitization at 0–2 years old(group 1: OR=0.18,95% CI=0.09–0.35;P≤ 0.001) was found to be as a protective factor for EW in the univariable risk analysis.
Risk factors for the development of dry cough at 9–11 years of age
Risk factors in the univariable risk analysis for DC at 9–11 years old are listed in the Table 4.Male gender(OR=1.95,95% CI=1.00–3.79;P=0.032),having eczema at 0–2 years old (OR=4.63,95% CI=2.40–8.91;P≤ 0.001),group 2 (OR=6.00,95% CI=1.06–33.73;P=0.042),group 4 (OR=7.38,95% CI=2.17–25.09;P≤ 0.001),group 5(OR=6.42,95% CI=1.85–22.29;P=0.003),group 7(OR=4.62,95% CI=1.25–17.05;P=0.013),eosinophilia(≥ 4%;OR=2.03,95% CI=1.03–4.01;P=0.028) and elevated total IgE (OR=2.91,95% CI=1.52–5.59;P≤ 0.001)were found to be risk factors for DC.Caesarean section(P=0.428),maternal allergy (P=0.153),paternal allergy(P=0.146),and having sibling asthma (P=0.331),group 3 (P=0.650) and group 6 (P=0.055) did not show any associations with DC.Not having an allergic sensitization at 0–2 years old (group 1: OR=0.14,95% CI=0.07–0.29;P≤ 0.001) was found to be a protective factor for DC in the univariable risk analysis.
Adjusted risk factors for the development of current wheeze,exercise wheezing and dry cough
The binary logistic regression analysis was used to establish the independent risk factors for the development of asthma symptoms (CW,EW and DC).For this purpose,the variables with aP≤ 0.003 in the univariable risk analysis were selected.Having eczema at 0–2 years old,group 1 and group 4 for CW(Table 2),having eczema at 0–2 years old,group 1,group 4 and eosinophilia (≥ 4%) for EW (Table 3),and having eczema at 0–2 years old,group 1,group 4,group 5 and elevated total IgE for DC (Table 4),were selected as possible independent risk factors for the logistic regression models (P≤ 0.003).The presence of eczema at 0–2 years old was found to be animportant risk factor for the development of CW,EW and DC (OR=2.83,95% CI=1.54–5.23,P≤ 0.001;OR=2.71,95% CI=1.33–5.54,P=0.006;and OR=3.03,95% CI=1.47–6.25,P=0.003,respectively).Also,not having an allergic sensitization at 0–2 years old (group 1),was observed as a significant protective factor for the development of CW,EW and DC (OR=0.32,95% CI=0.15–0.70,P=0.004;OR=0.21,95% CI=0.10–0.44,P≤ 0.001;and OR=0.25,95% CI=0.10–0.59,P=0.002,respectively) (Table 5).
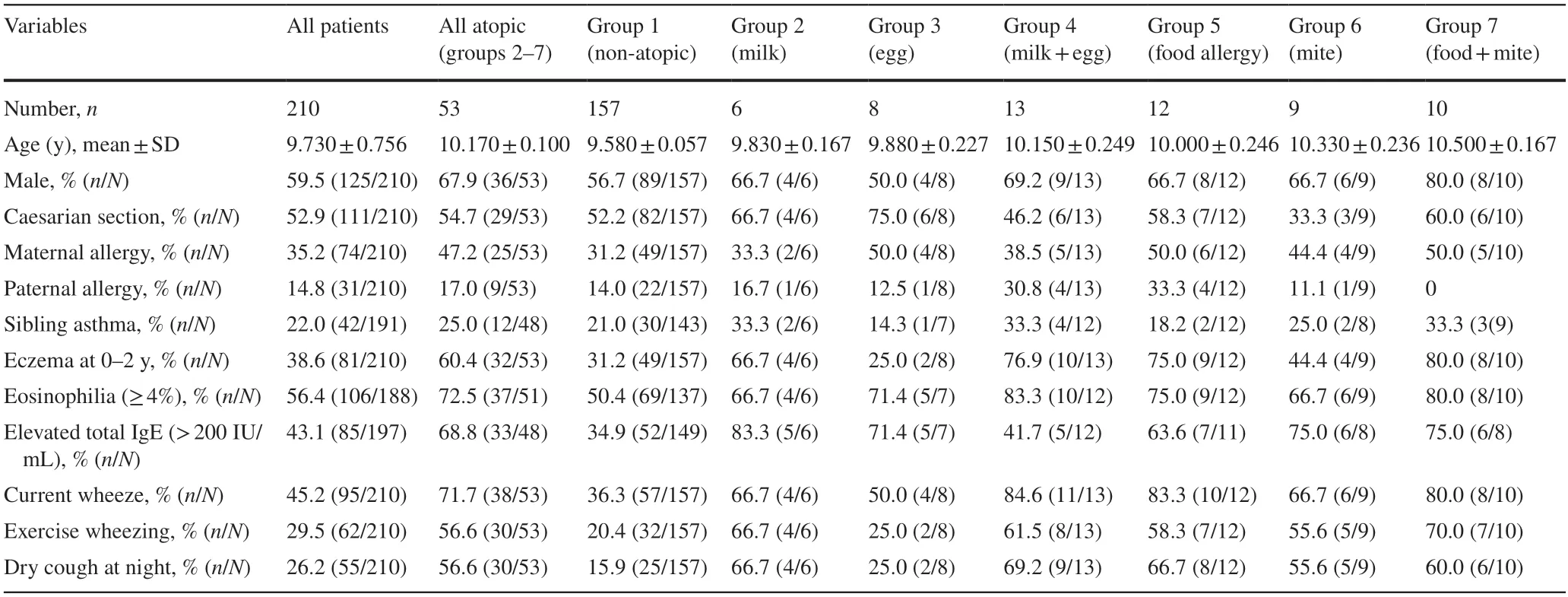
Table 1 Clinical characteristics of the groups
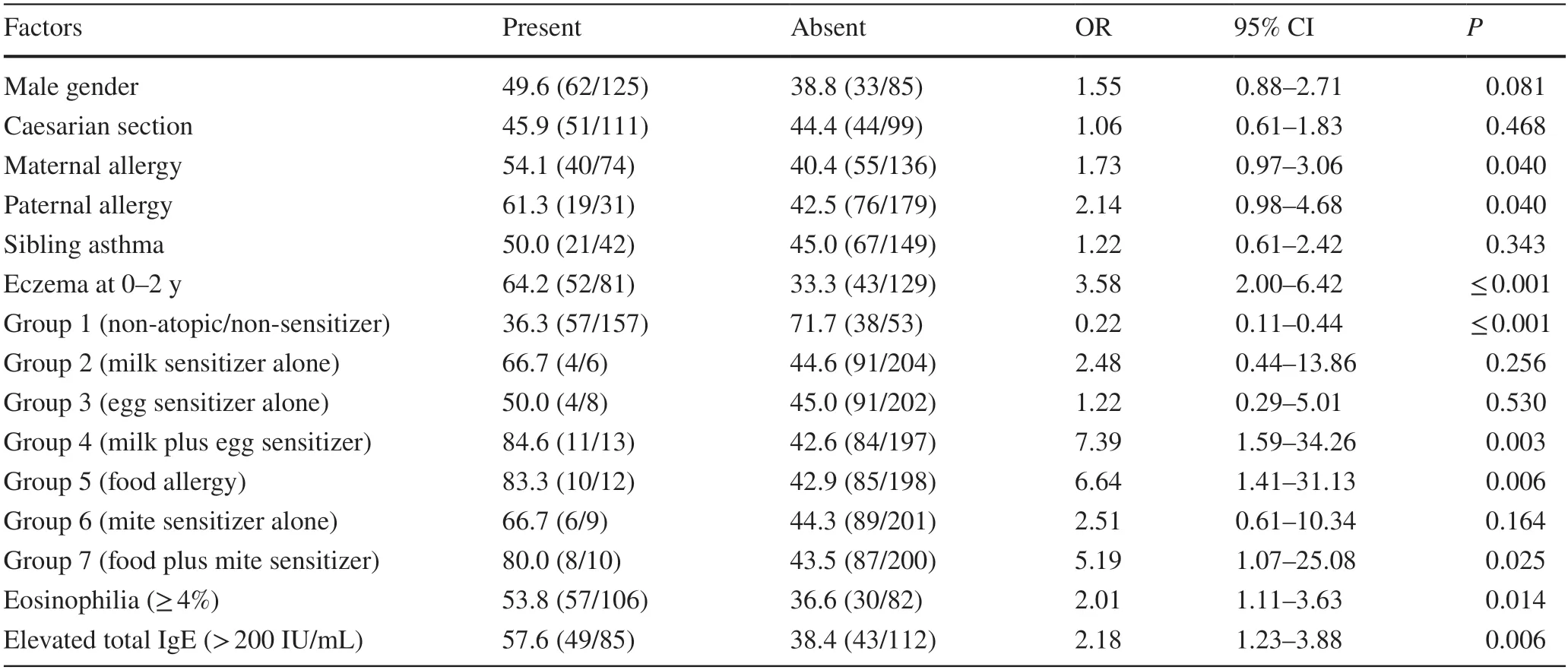
Table 2 Univariable risk analysis for current wheeze at 9–11 years of age
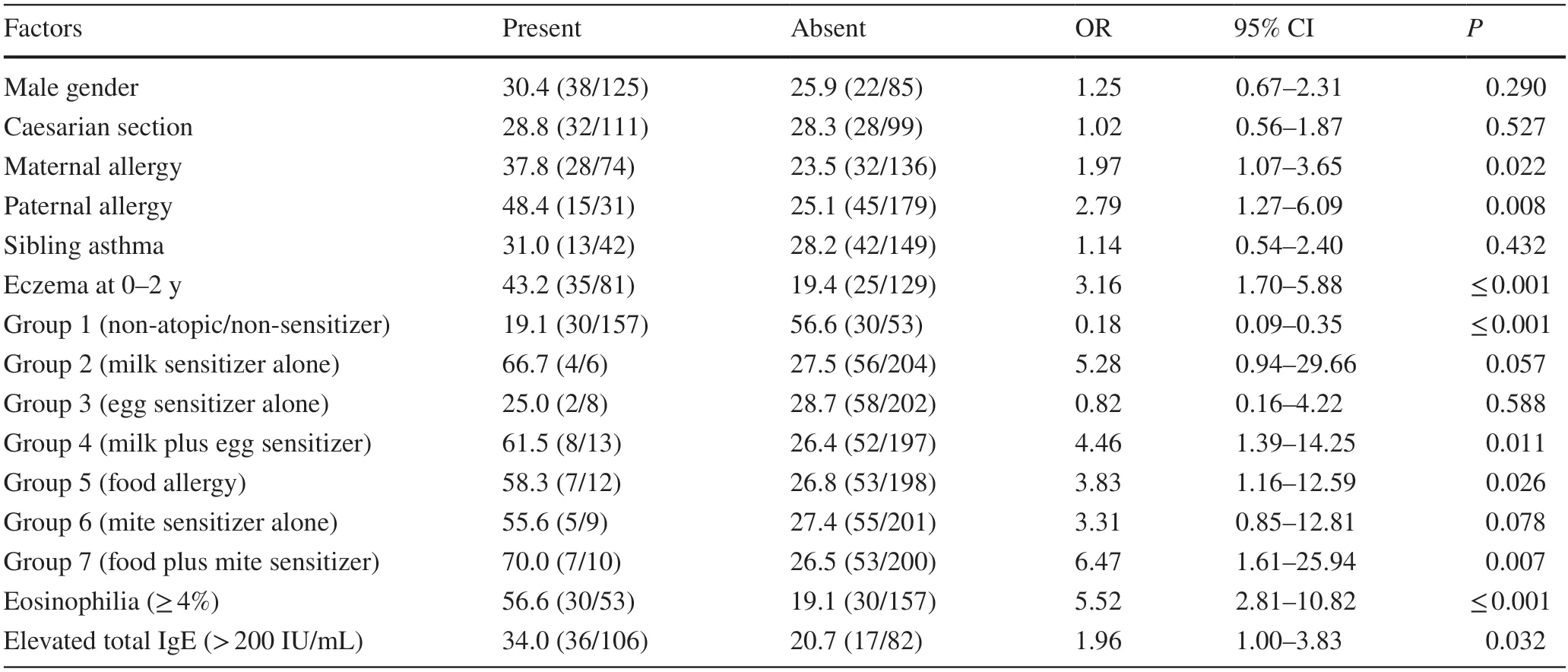
Table 3 Univariable risk analysis for exercise wheezing at 9–11 years of age
Discussion
The identification of risk factors associated with childhood asthma development remains an interesting area and is still a debated topic.In this study,we aimed to identify early life environmental risk factors that can be associated with development of asthma symptoms at 9–11 years of age.We found that asthma symptoms at 9–11 years old (CW,EW and DC)were associated with two independent factors in the study.
The first one,having eczema at 0–2 years old,was an important predisposing factor in development of all asthma symptoms (CW,EW and DC) at 9–11 years old.The concept of allergic multimorbidity supports those allergic diseases(asthma,rhinitis and eczema) tend to co-exist,suggesting common causal mechanisms amongst them.This is supported by evidence from the Mechanisms of the Development of Allergy study,which demonstrates coexistence of eczema,rhinitis and asthma in the same child is more common than what would be expected alone [9].The relation of one allergic disease to another is further supported by the atopic march paradigm,which describes the sequential progression from one allergic disease to another in the same individual.Typically,eczema tends to develop first,followed by IgE-mediated food allergy in early years of life,followed by allergic asthma and allergic rhinitis in later life years.The atopic march paradigm again proposes similar causal pathways amongst allergic disease or even suggests that one allergic disease may be causally leading to the next.However,many different factors have been proposed to be important in the atopic march process,including skin barrier dysfunction,allergic type 2 inflammation predisposition,presence to environmental triggers,such as allergens,microbes and pollutants,and oxidative stress.Additionally,the progression and severity of eczema,which we observed as an important risk factor for the development of asthma in our study,is dependent on various factors such as age of onset and family history of atopy,but also on presence of filaggrin mutations,polysensitization,and allergic multimorbidity [10,11].Early life eczema is defined as a major risk factor in the mAPI index.In addition,in the mAPI index the sensitizations of aeroallergens and food-allergens were defined as a major risk factor and a minor risk factor,respectively [6].Evidence from the Canadian Healthy Infant Longitudinal Development birth cohort showed that atopic dermatitis was associated with a seven-fold increased risk for asthma at 3 years but only if associated with allergic sensitization,whereas atopic dermatitis without allergic sensitization was not associated with an increased risk of asthma[12].Similarly,Gustafsson et al.[13],using data from a Swedish prospective study,demonstrated an increased risk for developing asthma in the children with eczema,particularly more severe eczema,and that early onset of eczema was associated with an increased risk of aero-allergen sensitization.The IoW birth cohort further showed that patients with filaggrin variants and allergic sensitization or eczema had a markedly increased risk of subsequent asthma by 4.93-fold(95% CI=3.61–6.71) and 3.33-fold (95% CI=2.45–4.51),respectively [14].The results of these studies support that eczema and allergic sensitization are important risk factors in the development of asthma in later life and are thus parallel to the results of our study.Different from our study in the medical literature,e.g.,Gaffin et al.[15],showed no association between eczema and asthma symptoms in children followed for at least 4 years.In this context,our study provides additional new evidence that having early personal eczema may be a significant risk for the development of asthma.
Not having an allergic sensitization at 0–2 years old(group 1) was found to be a protective factor (the second important result in the study) in the development of CW,EW and DC (Table 5) in this study.In other words,atopic sensitization at 0–2 years old was found to be an importantrisk factor in the asthma development at 9–11 years old.Atopic sensitization at early years of age has been thought to be an important risk factor for the development of childhood asthma.In this study,we observed that not having an atopic sensitization at 0–2 years old (group 1,n=157) has a significant protective effect on the development of asthma symptoms (CW,EW,DC) at 9–11 years old.In parallel with our results,in a prior published study,Kulig et al.[16],showed that children with persistent food sensitization had a 5.5-fold higher risk of developing asthma than infants who had transiently food sensitized at 0–2 years old.In another study,Rhodes et al.[17],showed that positive skin-prick test responses to hen’s egg,cow’s milk,or both in the first years was independently predictive of adult asthma.Christiansen et al.[18] also showed that both early transient and persistent sensitization to hen’s egg were associated with asthma and allergic rhino-conjunctivitis at 14 years old and also that transient sensitization to house dust mite similarly increased risk for asthma at 14 years old.Among similar studies,Illi et al.[4],showed that food sensitization alone (2.21-fold) and food plus aeroallergen sensitization (11.10-fold) at 0–2 years old were strong risk factors in the development of asthma at 7 years old.Kjaer et al.[19],showed early food sensitization (sIgE) at 3–18 months was found to be significantly associated with asthma at 6 years old.In the same study,early inhalant sensitization (sIgE) did not increase the risk of later allergic disease [19].Alduraywish et al.[20],using data from the Melbourne atopic cohort study and LISAplus (German population-based birth cohort) showed that co-sensitization to both food-and aero-allergens rather than single sensitization increases the risk for developing asthma and allergic rhinitis at 10–12 years old.
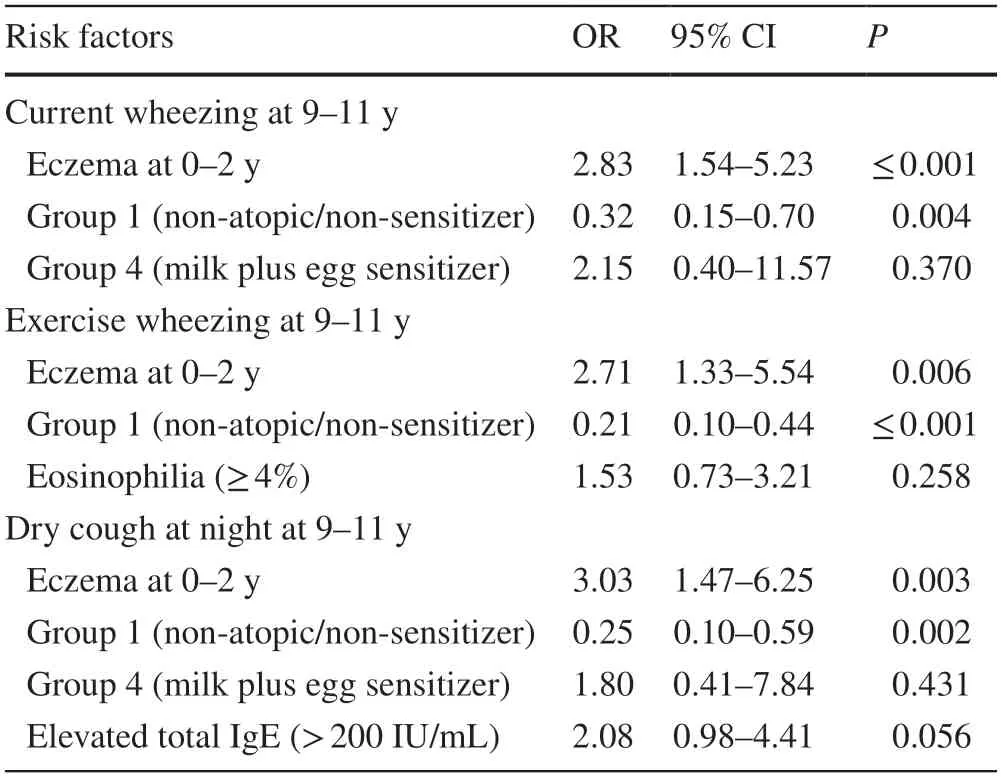
Table 5 Multivariable analysis for current wheeze,exercise wheezing and dry cough at 9–11 years old using binary logistic regression
In our study considering atopic subgroups (groups 2–7)separately,no subgroups had an influence on the development of asthma at 9–11 years old.In other words,at 0–2 years old,food-allergen sensitization alone (egg and milk,group 2 and group 3,respectively),multiple foodallergen sensitization (egg plus milk,group 4),food allergy(group 5),aero-allergen sensitization alone (mite,group 6),and food-allergen plus aero-allergen sensitization (egg and/or milk plus mite,group 7) had no effect on the development of CW,EW and DC at 9–11 years old.Similarly,we did not find any association between the history of parental allergies and sibling asthma with the development of asthma at 9–11 years old.There were no associations between current laboratory findings (eosinophilia,elevated total IgE)and asthma.We interpret that this situation may have been related to not having enough patients in subgroups.
This study has some limitations.First,the study was not a birth cohort study or a randomized controlled study that could provide more accurate information on the development of asthma.The second handicap of the study was the follow-up and that medical records of patients were not enough good.Also,because of there were long times between the first visit (0–2 years old) and the last visit(9–11 years old),the information of patients based on parental history (e.g.,eczema at 0–2 years old) may be not correct for every patient.The third limitation of the study was the small number of patients in all atopic subgroups.This situation may have affected the statistical significance.Also,the diagnosis of food allergy was based on only sIgEmeasurements in the group 5.Lack of oral food challenge tests in the diagnosis of food allergy was another limitation of our study.
In conclusion,having eczema and atopic sensitization at 0–2 years of age were observed as significant risk factors for all asthma symptoms (CW,EW and DC) at the age of 9–11 years.Having eczema at 0–2 years old was associated with a 2.83-fold,2.71-fold and 3.03-fold increased risk for CW,EW,and DC at 9–11 years old,respectively.Conversely,not having an atopic sensitization at 0–2 years old was associated with a 3.12-fold,4.76-fold and 4-fold reduction in risk for CW,EW,and DC at 9–11 years old,respectively (Table 5).A larger number of participant studies is needed to clarify risk factors associated with childhood asthma,especially in the atopic children.
Supplementary lnformationThe online version contains supplementary material available at https:// doi.org/ 10.1007/ s12519-022-00579-5.
Author contributionsAHH designed the study and collected data.NE and YY collected data.BB edited manuscript.All the authors approved the final version of the manuscript.
FundingNone.
Data availabilityThe data which analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethical approvalThis study was approved by the Ethics Committee of the Istanbul Health Sciences University,Kanuni Sultan Suleyman Training and Research Hospital (No.KAEK/2022.01.5).
Conflict of interestNo financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.The authors have no conflict of interest to declare.
 World Journal of Pediatrics2022年11期
World Journal of Pediatrics2022年11期
- World Journal of Pediatrics的其它文章
- Instructions for Authors
- Incident respiratory disease among youths using combustible tobacco,electronic nicotine products,or both: a longitudinal analysis
- Third-line therapies in patients with Kawasaki disease refractory to first-and second-line intravenous immunoglobulin therapy
- A novel HNF4A mutation identified in a child with maturity onset diabetes of the young
- Neutropenia: diagnosis and management
- Integration of multiscale entropy and BASED scale of electroencephalography after adrenocorticotropic hormone therapy predict relapse of infantile spasms